






Marc Darrow, MD, JD.
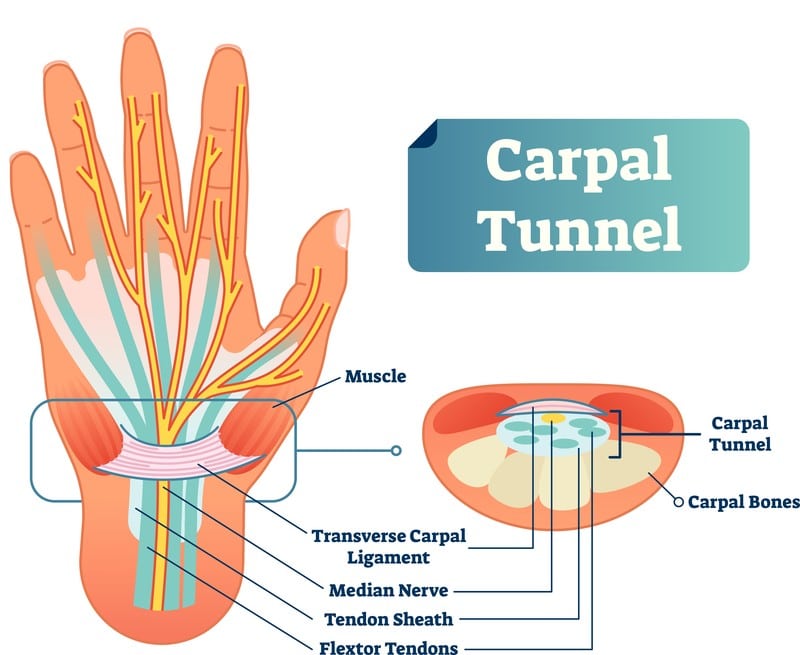
If you suffer from Carpal tunnel syndrome you know that it causes numbness, tingling, and pain in the wrist, hand and arm. You were probably told that you have a compression of the median nerve somewhere among the sea and ligaments of the wrist. For you, like many people, your condition may have worsened overtime. Traditional methods of treating Carpal Tunnel Syndrome include wearing a splint at night or injections of cortisone to reduce swelling were suggested.
Over the course of time you have tried:
- Ergonomic modification of office.
- Varying over the counter anti-inflammatories and pain medications.
- Wearing different wrist splints and braces.
- Exercise and physical therapy.
- Steroid injections.
Through your medical journey you may have been given Electrophysiological tests to the degree of median nerve impairment in carpal tunnel syndrome. This would include:
- Nerve conduction studies (NCS).
- Electromyogram (EMG).
If these measures are not successful, carpal tunnel release surgery, which sections the tough transverse carpal ligament and relieves pressure on the median nerve, may be performed. Despite some people having good success with surgery, there have been many patients who have presented to my office with worse symptoms after they had the carpal tunnel surgery.
Before we discuss conservative care let’s discuss Carpal Tunnel Syndrome in relationship to other problems in the hand.
Is there a connection between carpal tunnel syndrome and trigger finger?
A May 2020 study (6) reviewed the connection between Carpal tunnel release and trigger finger. The authors of the study wrote: “Carpal tunnel release is acknowledged as a predisposing factor for the development of the trigger finger. However, the incidence of new-onset trigger finger after Carpal tunnel release surgery has been inconsistently reported. In this study, we aimed to evaluate the prevalence of Carpal tunnel release as a risk factor of the development of the trigger finger.”
- Post-Carpal tunnel release trigger finger was detected in 26.3% of the 57 patients of this study
- The trigger finger occurred approximately six months after Carpal tunnel release surgery. The thumb and ring fingers were the most commonly involved fingers.
- Ten out of 15 (66.7%) patients who developed a post-Carpal tunnel release trigger finger had mild-to-moderate Carpal tunnel syndrome, and five (33.3%) patients had severe Carpal tunnel syndrome. No significant difference was found between the patients who did and did not develop a trigger finger after Carpal tunnel release surgery.
“The rate of developing a post-Carpal tunnel syndrome trigger finger was remarkable in our study.” The authors of this study suggested that patients under going Carpal tunnel release be advised of the potential of developing trigger finger.
Is there a connection between wrist and thumb osteoarthritis and Carpal Tunnel Syndrome
- In a study from March 2018 researchers found that degenerative osteoarthritis of the wrist was strongly associated with carpal tunnel syndrome.(13)
- In some instances surgeons will perform a thumb joint replacement and carpal tunnel release in the same procedure.(14)
Now, let’s look at the traditional conservative care route and make our way towards the surgery and see if along the way options can be found.
Traditional Conservative Care treatments for Carpal tunnel syndrome
A July 2022 study (1) compared the effects of radial extracorporeal shock wave therapy and local corticosteroid injection in patients with carpal tunnel syndrome
- A total of 72 patients who were diagnosed as having carpal tunnel syndrome were included in the study.
- One group received radial extracorporeal shock wave therapy,
- One group received the local corticosteroid injection
- The control group only used a resting hand splint.
Results:
- Both clinical and nerve conduction study parameters improved with all three groups, and this effect continued at the 12th-week follow-up of the patients.
- Pain, numbness and function scores improved in the first week after the treatment. At the 12th week after the treatment, these scores were significantly lower in the local corticosteroid injection group compared with the other two groups.
Low level laser therapy and corticosteroid injection
A June 2022 paper (2) compared the effects of low level laser therapy and corticosteroid injection in patients with moderate carpal tunnel syndrome (CTS).
- Eighty-seven patients (143 wrists) with moderate CTS were randomized to the corticosteroid or low level laser therapy groups. 40 mg of triamcinolone acetate solution was applied to carpal tunnel of 44 patients (74 wrist). Low level laser therapy was applied to 43 patients (70 wrist) five times a week, for a total of 15 sessions
- In both groups, median nerve intensity rate and palm function and pain improved significantly after the treatment. Based on this study, corticosteroid injection and low level laser therapy groups showed statistically significant difference at the 1st month (short-term), whereas there was no significant difference at the 6th month (intermediate-term).
A February 2022 study (3) assessed the effectiveness of manual therapy on pain, physical function, and nerve conduction studies in carpal tunnel syndrome patients. In this study the researchers examined six previously published outcome studies involving 401 patients. Reviewing these findings the research team concluded that their study: “highlights the effectiveness of manual therapy techniques based on soft tissue and neurodynamic mobilizations, in isolation, on pain, physical function, and nerve conduction studies in patients with carpal tunnel syndrome.
Carpal Tunnel Surgery
Study: Surgeons confident Carpal Tunnel Surgery is a good option for patients, but not for them. Surgeons less confident in the surgery if they, the surgeon, were the patient.
Here is a study from hand surgeons and post-surgical therapists.
Published in the Journal of plastic surgery and hand surgery, one of the objectives of this survey was to see if a surgeons’ eagerness to convince a patient of the benefit of six different surgical procedures differed if they, the surgeons themselves were recommended to get one of the six surgeries as a patient with hand/wrist pain. One of the 6 procedures was Carpal Tunnel Release.
- The surgeons in the study were divided into two groups.
- Group 1: Surgeons who were told to “pretend to be a patient being recommended to Carpal Tunnel surgery.”
- Group 2: Surgeons who were told to continue on being surgeons and make recommendations for Carpal Tunnel Syndrome treatments.
- The study’s findings: “Surgeons who considered themselves as patients had less confident perception on the benefit of carpal tunnel release compared with surgeons, who considered treating patients.”(4)
When can I return to work after carpal tunnel release surgery? Conflicting opinion causes problems for patients
Here is another problem with surgical intervention. Many people with carpal tunnel syndrome have it because of repetitive work related movements. So the question many of these people present to their surgeon is, “when can i go back to work?”
October 2018: The Journal of hand surgery, European volume. (5)
- In this study, over 300 surgeons and therapists responded to a request for what each one of them would recommend to a patient who asked: “When can I go back to work?,” following carpal tunnel release surgery
- The average recommendations were:
- 7 days for desk-based duties,
- 15 days for repetitive light manual duties and
- 30 days for heavy manual duties.
- However, the responses these patient received from their health care provider were wide-ranging:
- 0-30 days for desk-based;
- 1-56 days for repetitive light manual; and
- 1-90 days for heavy manual.
- The study authors suggested these variations were a problem: “Variation in the recommended timescales for return to work and other functional activities after carpal tunnel release suggests that patients are receiving different and possibly even conflicting advice.”
- The study’s conclusion: “There is a limited evidence base from which to derive recommendations for safe and effective return to different types of occupation after carpal tunnel release surgery.”
When can you return to work after carpal tunnel surgery? No one is quite sure.
Information on Carpal Tunnel Injections
A May 2024 paper (15) investigated the effectiveness of different injection therapies in alleviating the symptoms of carpal tunnel syndrome by reviewing 18 previously published studies. The data “revealed that platelet-rich plasma is effective in the treatment of carpal tunnel syndrome in terms of symptom and pain relief and functional improvement in both the short and long term, whereas steroids are effective only in the short term. Additionally, injections of dextrose solution (Prolotherapy) may offer long-term pain relief as well as short- and long-term symptom alleviation and functional improvement. The study findings suggest that platelet-rich plasma should be used as the first-line treatment for carpal tunnel syndrome, with dextrose and steroids serving as alternative treatment options.”
A March 2024 study writes: (16) “The best current evidence suggests that corticosteroid injections provide minimal transient improvement in nerve conduction and symptomatology compared with placebo or wrist splints.”
A September 2025 study published in Belgium (18) assessed treatment of patients with carpal tunnel syndrome (CTS), highlighting the use of the Boston Carpal Tunnel Questionnaire (BCTQ) for evaluating functional status and symptom severity, the visual analog scale (VAS) for measuring pain, and additional diagnostic methods such as electrodiagnostic studies and ultrasonography to assess median nerve characteristics. It concludes that while injection procedures are beneficial for patients with mild to moderate CTS, surgical treatment is generally more effective in improving both clinical outcomes and electrophysiological parameters.
Injection of simple dextrose more effective than cortisone
Cortisone is not considered a good long-term solution to Carpal Tunnel Syndrome. Studies show that any pain relief cortisone provides is short-lived.
In September 2018, (7) doctors compared cortisone injections against that of simple dextrose (Prolotherapy) and published their findings in the Annals of Neurology.
- Fifty-four people with mild-to-moderate carpal tunnel syndrome were randomly divided into a dextrose injection group and steroid injection group.
- The patients were administered one session of perineural injection with 5 cc of dextrose or 3 cc triamcinolone acetonide mixed with 2 cc normal saline (steroid group), under ultrasound guidance.
- Using various scoring tools, patients were assessed for response to treatment at 1, 3, 4, and 6 months post-injection.
RESULTS:
- All patients (27 wrists per group) completed the study. Compared with the steroid group, the dextrose group exhibited a significant reduction in pain and disability through 4th to 6th month.
- This study demonstrates that perineural injection of 5 cc of dextrose is more beneficial than that of corticosteroid in patients with mid-to-moderate carpal tunnel syndrome , 4 to 6 months post-injection.
A March 2024 paper, (17) assessed treatments in 92 wrists that were diagnosed as mild-to-moderate idiopathic carpal tunnel syndrome. The wrists were divided to receive a perineural corticosteroid injection therapy or 5% perineural dextrose (prolotherapy) injection with ultrasound guidance. The researchers found clinical and electrophysiologic improvement in carpal tunnel syndrome began from 1st month after perineural corticosteroid injection therapy and 5%PDIT. At the 6th month follow-up of the patients, 5% perineural dextrose (prolotherapy) injection and perineural corticosteroid injection therapy had similar therapeutic effects. As a result, we can consider the replacement of perineural corticosteroid injection therapy with 5% perineural dextrose (prolotherapy) injection in mild-to-moderate carpal tunnel syndrome patients especially in those who are hesitant because of the corticosteroid’s adverse effects.
Platelet Rich Plasma PRP injections and hydrodissection
- Nerve hydrodissection for carpal tunnel syndrome is a technique used when median nerve gets compressed in the wrist . It involves using an anesthetic or saline solution to separate the nerve from the surrounding tissue, specifically the tendon and fascia. We use a tiny needle under ultrasound guidance
A June 2022 study (8) tested the effects of hydrodissection in carpal tunnel syndrome. The researchers wrote: “Hydrodissection is an ultrasound-guided technique that has received more attention recently for its role in nerve entrapment syndromes. The purposes of this systematic review were to evaluate the safety and effectiveness of hydrodissection in carpal tunnel syndrome . . . (The researchers) concluded that nerve hydrodissection for carpal tunnel syndrome can be safely performed under ultrasound guidance. However, it is unclear whether the hydrodissection mechanism truly causes improvements in clinical outcomes.
A study from Athens University in Greece published in the journal Neural regeneration research (9) investigated whether a single injection of platelet-rich plasma would improve the clinical symptoms of carpal tunnel syndrome.
- Fourteen patients with median nerve injury who had suffered from mild carpal tunnel syndrome for over 3 months were included in this study.
- Under ultrasound guidance, 1–2 mL of platelet-rich plasma was injected into the region around the median nerve at the near edge of the carpal tunnel.
- At 1 month after single injection of platelet-rich plasma, results showed that pain almost disappeared in eight patients and it was obviously alleviated in three patients.
- Simultaneously, the disabilities of the arm, shoulder and hand questionnaire showed that upper limb function was obviously improved.
- In addition, no ultrasonographic manifestation of the carpal tunnel syndrome was found in five patients during ultrasonographic measurement of the width of the median nerve.
- During 3-month follow-up, the pain was not greatly alleviated in three patients of the 14 patients.
- These findings show very encouraging mid-term outcomes regarding use of platelet-rich plasma for the treatment of carpal tunnel syndrome.
Earlier in 2018,(10) the same researchers released similar findings in which they tested whether a single injection of platelet-rich plasma (PRP), under ultrasound guidance, can improve the clinical symptoms of patients with a mild to moderate carpal tunnel syndrome.
- In this study 50 patients suffering from mild to moderate carpal tunnel syndrome for a minimum of 3 months were randomly divided into 2 groups:
- Group A (26 patients) received an ultrasound-guided PRP injection into the carpal tunnel, whereas
- Group B (24 patients) was injected with placebo (0.9% normal saline).
- Group A patients demonstrated a 76.9% success in treatment whereas Group B patients demonstrated 33.3% success, which was significantly less than Group A
- The findings of this study suggest that a single PRP ultrasound-guided injection has positive effects in patients with carpal tunnel syndrome.
It appears PRP can be an effective treatment for Carpal Tunnel Syndrome as attested to by a December 2019 (11) which suggested: “PRP represents a promising therapy for patients with mild to moderate Carpal Tunnel Syndrome; however, included studies were limited as follow-up was short, the studies included patients that were heterogeneous, and the number of included studies was low.” Confirmation would come with more research.
A June 2021 study (12) tried to determine who could have a more successful PRP treatment and those who would be more challenging to treat. In this paper the researchers wrote: Platelet-rich plasma (PRP) injection is effective for mild-to-moderate carpal tunnel syndrome, and physicians have been using PRP injections to treat carpal tunnel syndrome. However, the predictive factors of PRP injections have not been evaluated. The research team noted that their retrospective study sought to identify the predictive factors of PRP injections in patients with moderate carpal tunnel syndrome.
- There were seventy-one patients with moderate carpal tunnel syndrome in this study. Each received a single PRP injection.
- The patient outcomes were recorded at the third- and sixth-month post-injection visits
- The patients were categorized into good and poor groups according to the following:
- (1) good outcome, with visual analogue scale (VAS) score decrease of more than 50% and
- (2) poor outcome, with VAS score decrease of less than 50% of pre-injection scores.
- The baseline body weight, distal motor latency, sensory nerve conduction velocity, and cross-sectional area of the median nerve were significantly different between the groups in the third month.
- Conclusion: Lower body weight, distal motor latency, and cross-sectional area of the median nerve values of the median nerve predict better outcomes after perineural injection of PRP for moderate CTS at the 3- and 6-month follow-ups.
A March 2026 study (19) examined the efficacy of platelet-rich plasma (PRP) injection, corticosteroid injection, and wrist splinting in patients with bilateral moderate CTS.
In this randomized controlled experiment, 45 patients with bilateral mild carpal tunnel syndrome were randomly allocated to one of three groups: PRP with splinting, corticosteroid injection with splinting, or splinting alone (as the control group). Assessments were conducted prior to treatment, as well as one month and six months after treatment began.
Pain scores in all groups improved significantly at both follow-ups. Notably, the PRP and corticosteroid groups demonstrated greater decreases in nocturnal discomfort and numbness than the control group. Strength assessments revealed improvement in all groups after one month; however, by six months, only the PRP group showed sustained enhancement in grip strength, while pinch strength benefits maintained in both the PRP and corticosteroid groups.
PRP, in particular, showed signs of greater sustained benefits, particularly at the six-month follow-up, implying that it may provide longer-term advantages.
An October 2025 study (20 ) revealed the findings of a comprehensive meta-analysis in 183 patients who underwent platelet-rich plasma (PRP) treatment. The results showed that patients in the PRP group had significantly lower symptom severity scores at 1, 3, and 6 months after treatment. Furthermore, at 3 and 6 months, the PRP group outperformed a conventional treatment control group in terms of functional status scores.
In terms of changes in the cross-sectional area of the median nerve, the PRP group showed a rise at one month, but decreased at three and six months. Despite these variances, there were no statistically significant differences between the PRP and standard treatment groups. Platelet-rich plasma is a safe and effective treatment option for carpal tunnel syndrome. PRP improves subjective outcomes, such as symptom severity and functional status, but has no effect on median nerve cross-sectional area, sensory nerve conduction velocity, and distal motor delay.
Call for a free phone consultation with our staff 800-300-9300
References
1 Dedes V, Tzirogiannis K, Polikandrioti M, Dede AM, Mitseas A, Panoutsopoulos GI. Comparison of radial extracorporeal shockwave therapy with ultrasound therapy in patients with lateral epicondylitis. Journal of Medical Ultrasonics. 2020 Apr;47:319-25.
2 Güloğlu SB, Filiz MB, Kılıç KK, Doğan ŞK, Toslak İE, Toraman NF. Treatment of carpal tunnel syndrome by low-level laser therapy versus corticosteroid injection: a randomized, prospective clinical study. Lasers in medical science.
3 Jiménez-del-Barrio S, Cadellans-Arróniz A, Ceballos-Laita L, Estébanez-de-Miguel E, López-de-Celis C, Bueno-Gracia E, Pérez-Bellmunt A. The effectiveness of manual therapy on pain, physical function, and nerve conduction studies in carpal tunnel syndrome patients: a systematic review and meta-analysis. International orthopaedics. 2021 Dec 3:1-2.
4 Leppänen OV, Jokihaara J, Jämsen E, Karjalainen T. Survey of hand surgeons’ and therapists’ perceptions of the benefit of common surgical procedures of the hand. Journal of plastic surgery and hand surgery. 2018 Jan 2;52(1):1-6.
5 Newington L, Francis K, Ntani G, Warwick D, Adams J, Walker-Bone K. Return to work recommendations after carpal tunnel release: a survey of UK hand surgeons and hand therapists. The Journal of Hand Surgery (European Volume). 2018 Jun 10.
6 Shafaee-Khanghah Y, Akbari H, Bagheri N. Prevalence of Carpal Tunnel Release as a Risk Factor of Trigger Finger. World Journal of Plastic Surgery. 2020 May;9(2):174.
7 Wu YT, Ke MJ, Ho TY, Li TY, Shen YP, Chen LC. Randomized double‐blinded clinical trial of 5% dextrose versus triamcinolone injection for carpal tunnel syndrome patients. Annals of neurology. 2018 Sep 5.
8 Neo EJ, Shan NT, San Tay S. Hydrodissection for carpal tunnel syndrome: A systematic review. American journal of physical medicine & rehabilitation.
9 Malahias MA, Johnson EO, Babis GC, Nikolaou VS. Single injection of platelet-rich plasma as a novel treatment of carpal tunnel syndrome. Neural Regeneration Research. 2015;10(11):1856-1859. doi:10.4103/1673-5374.165322.
10 Malahias MA, Nikolaou VS, Johnson EO, Kaseta MK, Kazas ST, Babis GC. Platelet‐rich plasma ultrasound‐guided injection in the treatment of carpal tunnel syndrome: A placebo‐controlled clinical study. Journal of tissue engineering and regenerative medicine. 2018 Mar;12(3):e1480-8.
11 Catapano M, Catapano J, Borschel G, Alavinia SM, Robinson LR, Mittal N. Effectiveness of platelet-rich plasma injections for nonsurgical management of carpal tunnel syndrome: a systematic review and meta-analysis of randomized controlled trials. Archives of physical medicine and rehabilitation. 2020 May 1;101(5):897-906.
12 Shen YP, Li TY, Chou YC, Chen LC, Wu YT. Outcome predictors of platelet‐rich plasma injection for moderate carpal tunnel syndrome. International Journal of Clinical Practice. 2021 Jun 9:e14482.
13 Bacle G, Marteau E, Corcia P, Garaud P, Laulan J. Are Carpal Tunnel Syndrome and Regional Degenerative Osteoarthritis Linked? Results of a Case-Control Study. The Journal of Hand Surgery (Asian-Pacific Volume). 2018 Mar;23(01):41-6.
14 Ingari JV, Romeo N. Basal Joint Arthroplasty and Radial-sided Carpal Tunnel Release Using a Single Incision. Techniques in hand & upper extremity surgery. 2015 Dec 1;19(4):157-60.
15 Yang FA, Wang HY, Kuo TY, Peng CW, Liou TH, Escorpizo R, Chen HC. Injection therapy for carpal tunnel syndrome: A systematic review and network meta-analysis of randomized controlled trials. PloS one. 2024 May 16;19(5):e0303537.
16 Adindu E, Ramtin S, Azarpey A, Ring D, Teunis T. Steroid versus placebo injections and wrist splints in patients with carpal tunnel syndrome: a systematic review and network meta-analysis. Journal of Hand Surgery (European Volume). 2024 Mar 28:17531934241240380.
17 OCEK O, GUNER D. Perineural 5% dextrose versus corticosteroid injection in non-surgical carpal tunnel syndrom treatment. Clinical Neuroscience/Ideggyógyászati Szemle. 2024 Mar 30;77.
18 Kiratlioğlu Y, Kiratlioğlu E, Armangil M, Yoğun Y, Aksun ZÖ, Şener HÖ, Bezirgan U. Comparison of surgical treatment for Carpal Tunnel Syndrome with corticosteroid injection and platelet-rich plasma injection. Acta orthopaedica Belgica. 2025 Sep;91(3):299-307.
19 Cansever Ü, Doğan ŞK, Toslak İE, Filiz MB, Toraman NF. Comparison of the effectiveness of platelet-rich plasma (PRP) injection and steroid injection in patients with bilateral moderate carpal tunnel syndrome: a prospective randomized controlled trial. Injury. 2026 Jan 9:113018.
20 Du Y, Jiang X, Fu K, Cui C. Efficacy and safety of platelet-rich plasma in the treatment of carpal tunnel syndrome: A meta-analysis. Medicine. 2025 Oct 31;104(44):e45010.