






Marc Darrow, MD, JD.
Often we will hear from people who have had a hip arthroscopic surgery who have continued pain following the procedure. These people are now in a situation where they have to decide on three different courses of action. Redo the surgery, find other treatment options, or just manage the pain and live with it. Many orthopedist surgeons will try to find ways to address these patient’s concerns without immediately going back to hip surgery.
For someone who is active, surgery can be a confusing option. On the one hand, surgery is seen as an attractive option because there is a promise that the patient will be able to resume normal sporting activities quicker if they do not wait. Labrum tear and impingement is something, they are told, that will not heal on its own. On the other hand, surgical recovery can take a long time. Then there is the thought that the surgery may not be that successful.
So what is this person doing in our office? Are they trying to avoid the surgery, or worse, had they already had the surgery and the surgery did not provide the results that they had hoped for?
Types of Arthroscopic hip surgery
Once the MRI has determined a labral tear and the start of the bony overgrowth (osteoarthritis) the treatment options begin to narrow to cortisone to provide temporary relief and ultimately arthroscopic surgery to shave down and trim up the labrum’s soft tissue.
- arthroscopic debridement, (the trimming down of damaged soft tissue and washing out of bone chips or fragments),
- microfracture or drilling, (hip microfracture surgery is a common arthroscopic procedure where an awl (a sharp pointed tool) is pushed into the bone where the protective hip cartilage has worn away. The small holes made by the awl are called microfractures. The goal of this surgery is to build new cartilage by bringing the blood from the bone marrow into the hip joint to form a protective scab and fill in the cartilage defects.)
- Cartilage transplants or osteochondral allografting. or OATS: In this procedure, surgeons transfer a small piece of cartilage and bone from a healthy area to the damaged area For larger damaged areas of the hip cartilage, doctors may use allografts, or donated tissue.
What is causing the post-hip arthroscopy pain?
According to some surgeons, the pain can be coming from sources that were present before the surgery. In some cases then, the surgery did not address the cause of the pain. These other sources of pain could be coming from the SI joint, the low back, the pelvic area or from Piriformis syndrome.
An editorial by F. Winston Gwathmey in the journal Arthroscopy (1) suggested: “The increasing use of hip arthroscopy has been accompanied by an associated increase in revision hip arthroscopy. The results of revision surgery are generally inferior to primary hip arthroscopy. When revision hip arthroscopy fails, repeat revision hip arthroscopy may be indicated. Addressing the etiology of failure of the primary and first revision surgery is fundamental to achieving optimal outcomes in repeat revision cases. Unfortunately, poorly executed previous surgery is the leading etiology of failure, with unaddressed femoroacetabular impingement, hip labral damage, and capsular deficiency most commonly encountered during repeat revision surgery.”
Latest research:
A January 2024 paper (2) reviewed previously published data on risk of needing total hip replacement after hip arthroscopy. The researchers found: “Prior hip arthroscopy is a risk for postoperative dislocation, reoperation, or revision after conversion total hip replacement.”
Recently, a leading surgical center, the Hospital for Special Surgery says this: “The percentage of patients with hip arthritis who had a hip replacement within two years of hip arthroscopy was unacceptably high at 68%, according to a new study of more than 2,600 patients by investigators at Hospital for Special Surgery (HSS). Prior hip arthroscopy was also associated with significantly worse outcomes after hip replacement.”
“Arthroscopic hip surgery should not be performed in patients with a diagnosis of osteoarthritis”
This conclusion warning that people with hip osteoarthritis should not have arthroscopic surgery comes from Hospital of Special Surgery research published in the journal Hip International.(3) Here is the concluding remarks of that research:
“Analysis of a large insurance database found the conversion rate from hip arthroscopy performed in Medicare osteoarthritis patients to total hip replacement within 2 years is unacceptably high. Hip arthroscopy prior to total hip replacement also significantly increased the risk of total hip replacement revision within 2 years after index arthroscopic hip surgery . These results suggest that arthroscopic hip surgery should not be performed in patients with a diagnosis of osteoarthritis as conversion rates are high and revision rates post total hip replacement are significantly increased.”
A November 2023 study (4) found that older or middle age patients with smaller joint space width (more osteoarthritis) of the hip was associated with patients who were converted to total hip replacement following hip arthroscopy.
One study suggests complication not as high
A September 2022 paper (5) however found complication rates no higher in arthroscopic patients than control subjects following total hip replacement: “After elective total hip replacement, patients with prior hip arthroscopy exhibited significantly lower rates of medical complications and prolonged opioid claims within 90 days and prosthetic joint infection at 1 year. Rates of all other prosthesis-related complications within 2 years were statistically comparable (to those who did not have surgery).
If you have been recommend to a hip arthroscopic procedure you know why it was recommended. You had been diagnosed with femoroacetabular impingement, or to clean up some cartilage damage, a lot of people get the surgery to fix labrum tears, tendon problems or problems of bursitis. You were recommended to the surgery because you still had pain after your tried:
- Over the counter anti-inflammatories and pain relievers.
- A lot of icing.
- Balms and ointments.
- Physical therapy and stronger doses of anti-inflammatories.
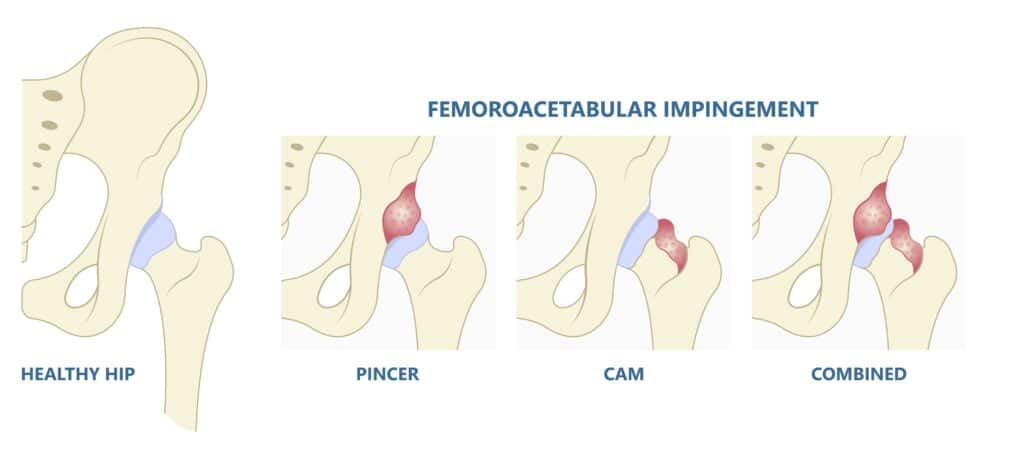
- And finally an MRI may have revealed enough damage to suggest a future a labral tear and the possibility of Femoroacetabular Impingement? (Bone spur formation that is pinching at the the hip labrum).

Reasons for hip arthroscopic failure
An October 2021 study (6) reported overall complication rate in hip arthroscopy was 7.3% (67/908 cases), the minor complication rate of 4.9% (45/908 cases) and the major complication rate 2.4% (22/908 cases). The most common severe complications were iatrogenic cartilage damage and instrument breakage, while the most common minor complications were perineal hypoaesthesia (loss of feeling or numbness in the buttocks, thighs and groin area) and heterotopic ossifications. The conversion rate to total hip replacement was 4.2% (39/908 patients).
The wrong surgery
- The wrong surgery: Many patients who have failed hip arthroscopic failure suffer from hip osteoarthritis. A 2021 study (7) noted: “Most patients had pre-existing osteoarthritis and/or chondral lesions that became apparent at arthroscopy.” It was then that doctors realized a hip replacement may have been more suitable. Hip arthroscopy is typically not helpful for osteoarthritis. Despite many patients being recommended to the arthroscopic surgery.
Not completely correcting a femoroacetabular impingement
is the leading cause of failed hip arthroscopy
A July 2021 paper in the journal Frontiers in surgery (8) discusses some of the aspects of a failed hip arthroscopy surgery:
“Hip arthroscopy is a reproducible and efficacious procedure for the treatment of femoroacetabular impingement syndrome. Despite this efficacy, clinical failures are observed, clinical entities are challenging to treat, and revision hip arthroscopy may be required.
The most common cause of symptom recurrence after a hip arthroscopy that leads to a revision arthroscopy is residual cam morphology as a result of inadequate femoral osteochondroplasty and restoration of head-neck offset, (this describes a procedure that shaves bone the neck of the femoral head or “ball” of the hip joint) though several other revision etiologies including progressive chondral (cartilage) and labral pathologies also exist. In these cases, it is imperative to perform a comprehensive examination to identify the cause of a failed primary arthroscopy as to assess whether or not a revision hip arthroscopy procedure is indicated.”
Femoroacetabular Impingement Syndrome is usually not an isolated diagnosis when the patient presents with chronic hip pain. It is part of a larger hip problem that can include muscle weakness and atrophy, advancing osteoarthritis, labrum tears, cartilage tears and ligament laxity or weakness. It is one or many or even all of these other factors that may contribue to post-arthroscopic hip pain.
Ligamentum teres tears
The ligamentum teres is a somewhat thick, cord like structure that connects the femoral head (the ball) to the acetabulum (socket). It functions to help hold the ball of the joint in place within the socket. A tear of the ligamentum teres is often found in patients with co-conditions of femoroacetabular impingement and labrum tear.
People with ligamentum teres tear typically feel pain when they do any activity that brings their knees towards their chin, such as walking up stairs, getting in and out of a car or chair. A compounding and confusing aspect of this type of injury is that it can cause a sensation of pain in the groin.
So why all the talk about the ligamentum teres?
There is a discussion in the medical community as to the importance or non importance of surgical reconstruction of the Ligamentum teres and its involvement in failed hip arthroscopic surgery.
An editorial commentary in the journal Arthroscopy (9) outlines these concerns:
“Ligamentum teres (LT) tears are correlated with hip instability, and biomechanical research suggests there is a stabilizing function of the intact native Ligamentum teres. With regard to Ligamentum teres reconstruction, currently, there are imaging studies demonstrating that the ligament goes on to heal and properly function. There are also no long-term clinical studies on the success rates of Ligamentum teres reconstruction. The clinical studies that have been done are done with a fairly high number of concomitant procedures, which makes it difficult to discern whether improvement can be attributed to the Ligamentum teres reconstruction. A recent review shows that after Ligamentum teres reconstruction, these very difficult patients can respond favorably to surgery two-thirds of the time. However, in the remaining one-third of patients, an additional surgery was required. . . For those not a candidate for periacetabular osteotomy , the patient should be educated on the risks of failure of Ligamentum teres reconstruction and have reasonable expectations, and the operation should be performed by an experienced hip arthroscopist with Ligamentum teres reconstruction.”
Arthroscopic surgery for hip labrum tears has its successes and its failures.
We are going to start with research in 2015 and bring it to 2014. You will see the problems of 2015 remain the problems of 2024.
In a recent study in the journal Sports medicine and arthroscopy review, (10) surgeons wrote of the benefits of hip labrum surgery. But watch how the study concludes, which I reproduced here, there may be a better way:
“The techniques utilized for the management of articular cartilage and labrum injuries during hip preservation surgery have changed dramatically recently . . .The overarching goal of labral treatment is to restore the native functions of the labrum to allow for more normal biomechanical function. Similarly, cartilage injuries can be managed a number of different ways, including with debridement, microfracture or drilling, cartilage transplants, and higher level restorative techniques. These cartilage restoration techniques have evolved rapidly as well, and may include the use of scaffolds, allograft cartilage cells, and other stem-cell-related procedures.)
The surgical options. Why aren’t they as good as hoped for?
Doctors in Japan reported these findings in January 2017 in the Journal of orthopaedic surgery and research. (11) These finding present a more pessimistic outlook of the surgical outcome:
Active person over 50 – One in 3 will go on to hip replacement
“Many studies have examined the clinical outcomes of arthroscopic surgery for treatment of hip labral tear and/or osteoarthritis in patients over 50 years of age. Overall these studies show that clinical outcomes generally improved, however they contained cases in which conversion to total hip replacement occurred at a constant rate. In the current study, 34.8% of the patients showed a progression to osteoarthritis AFTER arthroscopic procedures.”
There are no clear cut choices in surgery – You need a surgery to see if you need surgery
In March 2017, American Hip Institute researchers presented a paper (12) that suggested:
“Currently, three commonly practiced labral treatments are available: repair (surgical), débridement, and reconstruction. Arguments for and against each treatment option exist in the literature. Reviewing the currently proposed indicators for labral tear treatments in conjunction with the treatment procedures yields a thorough decision-making guide for choosing the appropriate labral procedure.There are no clear cut choices in surgery.”
A September 2018 study in the Orthopaedic journal of sports medicine (13) suggested:
“The intraoperative appearance of the labrum is the most important factor affecting surgical decision making. However, different surgeons viewing the same tear arthroscopically may select different treatments. The indications to repair a torn acetabular labrum are highly variable among hip arthroscopic surgeons.”
The vicious cycle. The second surgery is not as good as the first.
You get the second surgery because the first one failed
In January 2020, James D. Wylie, MD wrote an editorial in the medical journal Arthroscopy. (14) This is what he wrote:
“Hip arthroscopy has evolved significantly over the last 5 to 10 years. With this comes the burden of patients with continued pain after their index (first) procedure. Reasons for the need for revision surgery can be many, including incomplete resection of impingement morphology, unrecognized/unaddressed acetabular dysplasia or hip instability, failure to manage the soft tissue appropriately (i.e., labrum or capsule/ligament), or other unrecognized cause of pain, like femoral retroversion (the femoral head is not in the correct position, a tell tale sign is that the foot is pointed outward) or subspine impingement. Like many other orthopaedic procedures, revision hip arthroscopy with or without a defect in the hip capsule has significantly worse outcomes at 2 years compared with primary hip arthroscopy. This emphasizes the importance of proper diagnosis, well-done surgery, and proper rehabilitation the first time to avoid the need for revision hip surgery in the young adult altogether.
In April 2020 another editorial in the medical journal Arthroscopy (15) made these comments that pain management after the procedure is lacking.
“Pain after hip arthroscopy is a significant and challenging issue as is evidenced by the number of publications on this subject. Various analgesic strategies to circumvent this issue have been tried, with variable results. The central problem is that pain experienced by patients after hip arthroscopy is multifactorial in origin. Regarding local injection, an anatomic approach to the nerve supply to the hip with an effective pain relief strategy should take this into consideration and focus on using drugs with a low risk of complications and infiltration techniques that do not cause an unnecessary delay in rehabilitation and discharge of the patient. Furthermore, addressing traction time, surgical technique, and fluid extravasation and applying an individualized approach, keeping the patient’s personality and profile in mind, will ensure adequate analgesia after arthroscopic intervention.”
And also from April 2020, from the The American journal of sports medicine.(16)
“While the indications for primary hip arthroscopic surgery in treating femoroacetabular abnormalities continue to be defined, the indications and outcomes for revision hip arthroscopic surgery remain ambiguous. However, revision hip arthroscopic surgery is performed in 5% to 14% of patients after their index procedure. While patient-reported outcomes (PROs) generally improve after revision procedures, the extent of their improvement is not well defined. . . “
The researchers also note that after revision hip arthroscopic surgery, studies have suggested the rates of conversion to total hip replacement ranged up to 14.3%, and the rates of further arthroscopic revision ranged also ranged to 14% of patients.
In a March 2022 paper (17) researchers noted that “Although surgical procedures to treat Femoroacetabular impingement (FAI) led to satisfactory outcomes, there was a revision rate of 5.29% in the 9357 procedures in (this study). The rate of progression to total hip replacement after a median follow-up of 30 months was 3.78%. Patients who have a higher BMI (overweight) and/or have a pathologic acetabular index and/or undergo labral debridement during correction of Femoroacetabular impingement are more at risk for a subsequent total hip replacement. (The authors) advocate additional education of this patient population in terms of expected outcomes and suggest surgical labral repair instead of debridement if needed.”
From hip arthroscopy to hip replacement
In a patient outcome summary of 5048 patients, a February 2024 study (18) identified rates of conversion from hip arthroscopy to hip replacement.
- 12.86% for isolated debridement,
- 8.67% for isolated labral repair, and,
- 6.76% for femoroacetabular osteoplasty.
The authors of the study also noted: “Older patients and those with preexisting osteoarthritis of the hip were at a significantly increased risk of failing hip arthroscopy and requiring a total hip replacement within 2 years of the (hip arthroscopy.) Younger patients were at low risk of requiring a conversion procedure no matter which arthroscopic procedure was performed.
Does hip arthroscopy increase risk of hip replacement complication, especially dislocation?
A January 2024 paper (19) examined this question. The study authors wrote: “The indications for hip arthroscopy have been increasing, as have been the number of patients undergoing total hip arthroplasty (replacement) after hip arthroscopy. Several matched cohort studies have assessed the impact of prior hip arthroscopy on total hip arthroplasty, but conflicting results have been observed.”
To help clarify the question, the researchers performed an updated systematic review and meta-analysis and their findings confirmed that prior hip arthroscopy affected the overall rate of complications after subsequent total hip replacement, especially the odds for dislocation.
Does hip arthroscopy increase risk of hip replacement complication, especially dislocation?
Traditional treatment options
As I mentioned above, surgeons will typically recommend a conservative non-surgical management plan for patients with persistent pain after failed hip arthroscopy. These treatments would include NSAIDs (anti-inflammatory medications), cortisone or corticosteroid injections and physical therapy. Patients would also be asked to avoid movement or activity that would aggravate their pain. This would include some exercises and stretching like yoga.
It should be pointed out that many of these conservative care options were used by the patient before they were recommended to surgery and it was the failure of these treatments that send them to hip surgery in the first place. It is because of this and the nature of post-surgical damage in the hip that these conservative care options fail at high rate and send the patient to a revision surgery.
Injection treatments and hip preserving surgery
I have written articles, which you can see on this website on cortisone injections and viscosupplementation / hyaluronic acid.
- PRP treatments involve collecting a small amount of your blood and spinning it in a centrifuge to separate the platelets from the red cells. The collected platelets are then injected into toe joints to stimulate healing and regeneration.
- Bone marrow derived stem cells. These stem cells are also injected into to the joint to stimulate healing and regeneration.
The determination of which method is used is made during the initial consultation and physical examination of the hip.
In May 2019, doctors at the Mayo Clinic published research on ultrasound guided platelet rich plasma injections for treatment of symptoms associated with acetabular hip labral tears. What the Mayo Clinic researchers hoped to answer was whether PRP was safe and effective. The results were published in the American journal of physical medicine & rehabilitation.(20)
- The researchers looked at 8 patients who have previously failed conservative management and received ultrasound-guided injection of PRP at the site of hip labrum tear. The patients were assessed for pain and functionality at the start of treatment, then 2, 6, and 8 weeks after injection.
- The findings: Results were good, improvements in pain and function were seen at the 2, 6 and 8 week marks post injection.
- The conclusion: “Ultrasound-guided injection of PRP holds promise as an emerging, minimally-invasive technique toward symptom relief, reducing pain, and improving function in patients with hip labral tears.”
Call for a free phone consultation with our staff 800-300-9300
Information on Femoroacetabular Impingement Syndrome treatments
Do corticosteroid injections accelerate the need for hip replacement?
References
1 Gwathmey FW. Editorial Commentary: Repeat Revision Hip Arthroscopy: Unaddressed Femoroacetabular Impingement, Labral Damage, and Capsular Deficiency Are Commonly Encountered. Arthroscopy: The Journal of Arthroscopic & Related Surgery. 2021 Dec 1;37(12):3442-4.
2 Arakawa H, Kobayashi N, Kamono E, Yukizawa Y, Takagawa S, Honda H, Inaba Y. Prior hip arthroscopy increases the risk of dislocation, reoperation, and revision after hip arthroplasty: An updated meta-analysis and systematic review. Journal of Orthopaedic Science. 2024 Jan 1;29(1):157-64.
3 Malahias MA, Gu A, Richardson SS, De Martino I, Sculco PK, McLawhorn AS. Hip arthroscopy for hip osteoarthritis is associated with increased risk for revision after total hip arthroplasty. HIP International. 2020 Mar 3:1120700020911043.
4 Dove JH, Laperche J, Schiller J, Tabaddor R, Cohen E. Older age and smaller joint space width are associated with conversion to total hip arthroplasty following hip arthroscopy. Journal of Orthopaedics. 2023 Dec 1;46:174-7.
5 Ross BJ, Wortman RJ, Lee OC, Mansour III AA, Cole WW, Sherman WF. IS PRIOR HIP ARTHROSCOPY ASSOCIATED WITH HIGHER COMPLICATION RATES OR PROLONGED OPIOID CLAIMS AFTER TOTAL HIP ARTHROPLASTY? A matched cohort study. Orthopaedic Journal of Sports Medicine. 2022 Sep 29;10(9):23259671221126508.
6 Zeman P, Rafi M, Kautzner J. Evaluation of primary hip arthroscopy complications in mid-term follow-up: a multicentric prospective study. International Orthopaedics. 2021 Oct;45:2525-9.
7 Vesey RM, Bacon CJ, Brick MJ. Pre-existing osteoarthritis remains a key feature of arthroscopy patients who convert to total hip arthroplasty. Journal of ISAKOS. 2021 Jul 1;6(4):199-203.
8 Kunze KN, Olsen RJ, Sullivan SW, Nwachukwu BU. Revision hip arthroscopy in the native hip: a review of contemporary evaluation and treatment options. Frontiers in surgery. 2021 Jul 5;8:662720.
9 Hartigan DE, Hegedus CE. Editorial Commentary: Ligamentum Teres Reconstruction May Improve Hip Stability But Has High Revision Rates: Fad or Restoration of Function?
10 Salata MJ, Vasileff WK. Management of Labral and Chondral Disease in Hip Preservation Surgery. Sports medicine and arthroscopy review. 2015 Dec 1;23(4):200-4.
11 Moriya M, Fukushima K, Uchiyama K, et al. Clinical results of arthroscopic surgery in patients over 50 years of age—what viability does it have as a joint preservative surgery? Journal of Orthopaedic Surgery and Research. 2017;12:2. doi:10.1186/s13018-016-0504-9.
12 Domb BG, Hartigan DE, Perets I. Decision making for labral treatment in the hip: repair versus débridement versus reconstruction. JAAOS-Journal of the American Academy of Orthopaedic Surgeons. 2017 Mar 1;25(3):e53-62.
13 Herickhoff PK, Safran MR. Surgical Decision Making for Acetabular Labral Tears: An International Perspective. Orthop J Sports Med. 2018 Sep 20;6(9):2325967118797324. doi: 10.1177/2325967118797324. PubMed PMID: 30263897; PubMed Central PMCID: PMC6149026.
14 Wylie JD. Editorial Commentary: The First Hip Arthroscopy Is the Best Hip Arthroscopy, Capsular Defect or Not. Arthroscopy. 2020;36(1):137–138. doi:10.1016/j.arthro.2019.09.009
15 Sardesai AM, Garner M, Khanduja V. Editorial Commentary: Pain After Hip Arthroscopy-Are We Truly Addressing the Problem?. Arthroscopy. 2020;36(4):1045–1047. doi:10.1016/j.arthro.2020.02.013
16 O’Connor M, Steinl GK, Padaki AS, Duchman KR, Westermann RW, Lynch TS. Outcomes of Revision Hip Arthroscopic Surgery: A Systematic Review and Meta-analysis. Am J Sports Med. 2020;48(5):1254–1262. doi:10.1177/0363546519869671
17 Tiao J, Ranson W, Ren R, Wang KC, Rosenberg AM, Herrera M, Zubizarreta N, Anthony SG. Assessment of Risk Factors and Rate of Conversion to Total Hip Arthroplasty Within 2 Years After Hip Arthroscopy Utilizing a Large Database of Commercially Insured Patients in the United States. Orthopaedic Journal of Sports Medicine. 2024 Feb;12(2):23259671231217494.
18 Arakawa H, Kobayashi N, Kamono E, Yukizawa Y, Takagawa S, Honda H, Inaba Y. Prior hip arthroscopy increases the risk of dislocation, reoperation, and revision after hip arthroplasty: An updated meta-analysis and systematic review. Journal of Orthopaedic Science. 2023 Jan 18.
19 Arakawa H, Kobayashi N, Kamono E, Yukizawa Y, Takagawa S, Honda H, Inaba Y. Prior hip arthroscopy increases the risk of dislocation, reoperation, and revision after hip arthroplasty: An updated meta-analysis and systematic review. Journal of Orthopaedic Science. 2024 Jan 1;29(1):157-64.
20 De Luigi AJ, Blatz D, Karam C, Gustin Z, Gordon AH. Use of platelet-rich plasma for the treatment of acetabular labral tear of the hip: a pilot study. American journal of physical medicine & rehabilitation. 2019 Nov 1;98(11):1010-7.