






Marc Darrow, MD, JD.
In this article I hope to share with you three main thoughts from recent research.
- Who is at risk for failed back surgery?
- What happens to put people at risk for failed back surgery syndrome before the surgery?
- What can be done in situations for failed back surgery syndrome after the surgery?
I have made it a point throughout this website to display my great admiration for surgeons. I went to medical school to become a surgeon. As I saw more and more failed surgeries I decided to change my practice over to providing non-surgical methods. There are very many people who have had very successful spinal surgeries.
We receive many emails from patients who have undergone numerous spinal procedures. These people are in continued pain and are looking for help. Because of the complexities of spinal surgery, especially in patients with numerous procedures, this question, “can regenerative medicine help me with my failed back surgery diagnosis?” must be answered following a physical examination and consultation where realistic healing options can be discussed.
Many people who have had a failed back surgery do not jump right back into another surgery. Many jump back into the conservative care loop that sent them to spinal surgery in the first place. Following failed back surgery the patient may be sent to physical therapy, get epidural steroid injections, get cortisone injections, be prescribed stronger painkillers and anti-inflammatory medications before they are told that another surgery may be needed. When a person contacts our office looking for options to a second or even third spinal procedure we do want to help them pursue a non-surgical path. Research has made it clear the more spinal surgeries, the worse off the patient is. This was also made clear to them by their own surgeons who warned them that the revision surgery they have planned may not work either and may make them even worse. Let’s explore the research in support of that statement.
Failed back surgery
A June 2024 paper (1) examined the causes and problems of failed back surgery syndrome. The paper points out there are many causes for failed back surgery. Among them: “Incorrect selection of the surgical procedure is a significant risk factor for failed back surgery syndrome. Performing decompression at the wrong level or single-level decompression without recognizing multilevel spinal involvement is unlikely to yield satisfactory outcomes. Inadequate lateral recess (not enough bone was removed) and neural foraminal decompression are significant causes of failed back surgery syndrome. Errors during spinal surgery can exacerbate preoperative pain and create new sources of pain. Poor surgical techniques can lead to segmental instability and increased pain resulting from direct nerve damage and intraoperative spinal cord ischemia.” Further, if the first surgery fails, the prospects for better success in a second surgery are as follows:
“Revision surgery is often recommended for patients with pain that is refractory (not responding) to other treatments and has an anatomical or pathological source identified by imaging. For example, chronic pain caused by recurrent disc herniation and adjacent segment degeneration usually requires surgical intervention. However, surgical revision is associated with significant morbidity, a higher risk of developing new neurological deficits, and low success rates, with insufficient evidence supporting its efficacy. Given the unsatisfactory outcomes of revision surgery, surgical treatment should be considered a limited therapeutic option. “
A July 2022 paper (2) describes failed back surgery syndrome treatment this way: “A number of factors underlie and maintain failed back surgery syndrome and successful management of pain chiefly depends on identifying them. Pharmacological, surgical, and non-surgical therapeutic measures are taken to treat the pain. Spinal cord stimulation and nerve stimulation have been widely practiced in this regard and enhanced pain reduction and patient satisfaction. In hernia and recurrent disc degeneration and sagittal imbalance, discectomy and/or fusion are indicated.”
Surgical decompression is recommended in carefully selected patients who do not improve after nonsurgical care. The use of additional fusion in surgery for degenerative spondylolisthesis has been a controversial issue. Arguments for fusion have included the assumption that pain arises from abnormal movement in the slipped segment and that this problem might worsen after decompression. In the past 3 decades, decompression with fusion has been the gold standard for treatment of patients with spinal stenosis with spondylolisthesis as well as for many patients without spondylolisthesis. However, current evidence indicates that the more invasive fusion procedure is associated with increased costs but not clinical benefits.
“The need for revision surgery declined but not because the first surgery was successful but because the second procedure was thought too risky”
The success of spinal surgeries is seen by some as a decrease in the need to have a second surgery. A second surgery implies in some patients that their first surgery has somehow failed. Recent research published in the Journal of Bone and Joint Surgery (3) looked at the reasons and likelihood that a patient would need a second spinal surgery for stenosis. One thing that they noted was that the need for revision surgery declined but not because the first surgery was successful but because the second procedure was thought too risky.
When I was in medical school, I did surgical research and assisted in the operating room much more than my classmates. By the time I had finished medical school and internship (where I spent as much time as possible doing orthopedic procedures) I had seen too many surgical failures including my own shoulder surgery. Worse was when the first surgery clearly failed, the patient was offered a second surgery to fix the first one. Older patients usually refused the second surgery, later documented in the research: “The likelihood of repeat surgery for spinal stenosis declined with increasing age and other diseases, perhaps because of concern for greater risks.” (4) There may have been less surgeries because older patients were not able to have them.
In another recent study (5) surgeons discussed treatment options for Failed Back Surgery Syndrome patients. One thing they discussed was in many cases revision or repair surgery were not viable options. They wrote:
“A significant number of lumbar post-surgical patients continue to suffer persistent pain and limited function and are termed to have “Failed back surgery syndrome” (FBSS). Treatments for FBSS may be generally categorized as physical therapy and exercise, medications, neuromodulation and re-operation. . . Evidence is weak for medications and re-operation, but strong for active exercise and interventional procedures such as adhesiolysis. (Surgery to removal scar tissue that resulted from the initial surgery).” Evidence remains week that surgery can fix a failed back surgery.
In April 2020, a study titled: “The Long-Term Reoperation Rate Following Surgery for Lumbar Stenosis,” found these statistics for lumbar stenosis surgery:(6)
- The overall cumulative incidence of reoperation for lumbar stenosis was:
- 6.2% at 2 years,
- 10.8% at 5 years and
- 18.4% at 10 years.
- The overall cumulative incidence of reoperation for anterior fusion was 20.6% at ten years post-op.
- The overall cumulative incidence of reoperation for posterior fusion was 12.6% at ten years post-op.
- The overall cumulative incidence of reoperation for decompression was 18.6% at ten years post-op.
Which patients are at higher risk for Persistent Spinal Pain Syndrome Type 2
– failed back surgery syndrome?

In recent years Persistent Spinal Pain Syndrome Type 2, that is pain from failed spinal surgery, has begun to replace failed back surgery syndrome as the diagnosis for pain after spinal surgery.
A September 2022 paper (7) looked at the surgical outcomes of over 100,000 spinal surgery patients. This is what they found as it relates to a failed back surgery classification.
Results:
- Of 102,047 patients who had lumbar fusion or decompression surgery (54% decompression procedures, 36% posterior fusions, and 8.9% anterior fusions) 5.4% of patients were diagnosed with failed back surgery syndrome within six months of the procedure, and 8.4% were diagnosed with failed back surgery syndrome within twelve months.
- High rates of failed back surgery syndrome occurred in in the elderly (age group 70-74).
- Among the surgical techniques, multi-level procedures had significantly higher rates of failed back surgery syndrome than single-level procedures, the highest being 10% in multi-level inpatient decompression procedures.
The general numbers of this study are that out 1 in 20 patients will develop failed back surgery in the first six months post-operation. This number will rise to about 1 in 12 within the first year of the surgery. Why are these numbers that high? Research suggests it is because inappropriate patients are getting surgery. Let’s follow that up.
An August 2022 paper (8) suggested: “The most common reasons for early reoperation (revision surgery within three months) and late operation (revision surgery after 3 months) were surgical site infection and adjacent segment diseases, respectively. Osteoporosis and diabetes were independent risk factors for early reoperation, and multilevel fusion was independent risk factor for late reoperation. Surgeons should pay more attention to these patients, and future studies should consider the effects of follow-up periods on results.”
Surgeons tell their fellow surgeons to warn their patients that their spinal surgery
will probably not help them as much as the patients may wish it would.
As we see in the above research, up to 1 out of 12 patients will have failed back surgery syndrome within one year of the surgery. There are many more patients whose outcomes did not meet their expectations.
In a 2018 study from the Netherlands (9), surgeons recommended that doctors do not refer many patients to spinal surgery who:
- Suffered from a degree of disability,
- already had 2 or more previous spine surgeries,
- psychosocial complaints, (the feeling of being unneeded, unwanted or burdensome)
- or if the patients were over 50, because the likelihood for the majority of them is that the surgery will not be helpful.
The theme here is the appropriateness of the patient. Patients who were not good candidates for surgery and have the surgery are at higher risk for the surgery failing. This is further outlined in an April 2022 paper (10) where patients who received a second opinion and were still recommended to surgery had better outcomes. In this study of 100 patients, 88 had a lumbar decompression, 12 had a lumbar fusion. Of interest is that between the first and second opinions, the two doctors agreed on what the diagnosis was only 44% of the time. Between the first opinion doctor and the second opinion doctor, only 27 agreed on a treatment recommendation. This study concludes: “the high rates of diagnostic and therapeutic indication disagreements corroborate the need of a second opinion in cases of spine disease with surgical indications.”
A January 2024 study (11) noted “over 60.0% of patients with low back pain (are) being referred to spine surgeons without any surgical indication. . . (this reveals) a significant proportion of inappropriate referrals to specialized care for low back pain.”
In this paper, 500 patient cases were analyzed, only 112 (22.4%) were surgical candidates, while 221 (44.2%) were discharge from the neurosurgery service upon initial assessment. . . . “over 80.0% of referrals made during the study period were deemed inappropriate. Inappropriate referrals were characterized by higher proportion of patients symptomatically improved, presenting a back-dominant chief complaint, exhibiting no objective neurological symptoms, and diagnosed with non-specific low back pain.”
Improvement in pain was the major expectation of patients undergoing lumbar spine surgery. For many, this was not achieved.
In a recent study, doctors at Weill Cornell Medical College in New York and the Hospital for Special Surgery, (12) discussed with patients what their pre-surgery expectations were and their satisfaction after the surgery. In other words, “how did the surgery turnout?”
The average age of this patient group was was 56 years old and 55% were men. Improvement in pain was the major expectation of patients undergoing lumbar spine surgery.
- Two years after surgery 11% of patients reported no improvement in pain, (1 out of 9)
- 28% reported a little to moderate improvement, (more than 1 out of 4)
- In total from first two groups 40 % of the patients report no, little or moderate pain relief
- 44% reported a lot of improvement,
- and 17% reported complete improvement.
This same warning is echoed in a recent study in the journal Pain Practice: (13) The patient-physician encounter forms the cornerstone of every health service. However, optimal medical outcomes are often confounded by inadequate patient-physician communication. Therefore, it is crucial to address all components of the patient’s pain experience, including beliefs and expectations.
Are spinal surgeries as successful as we think?
Factors before surgery that lead to risk of spine surgery failure
A December 2020 (14) study included 647 patients who had undergone lumbar spine surgery. Of these, 564 (87%) indicated that they were satisfied with the care they received. But did this translate to a better situation for the patient? One aspect that the researchers questioned was how pain was reported. In fact, how patients reported their pain may lead to skewed satisfaction scoring. The study notes: “pain-related outcome measures may serve as better predictors of patients’ satisfaction with their spine surgeons. Furthermore, this suggests that the current method by which patient satisfaction is being assessed and publicly reported may not necessarily correlate with validated measures that are used within the spine surgery setting to assess surgical efficacy.
A February 2023 study (15) explored why some patients had a failed lumbar decompression surgery with and without fusion. In this study of nearly 9000 patients, researchers found “After surgery for lumbar spinal stenosis, 33% of the patients reported failure, and 22% reported worsening . . . Preoperative duration of back pain for longer than 12 months, former spinal surgery, and age above 70 years were the strongest predictors for increased odds of failure and worsening after surgery.”
A group of Canadian doctors wrote in a July 2022 study (16) of the “complex relationship” between a patient’s pre-operative expectations of their spinal surgery, if those pre-surgery expectations were met, post-surgical outcomes, and satisfaction after spine surgery to help determine, what is a successful spinal surgery.
This study was conducted as a Canadian national study of patients undergoing elective surgery for degenerative spinal conditions
- Fifty-eight percent of patients were extremely satisfied, and 3% were extremely dissatisfied.
- Pre-surgery outcome expectations were variable and generally high.
- 17.3% of patients reported that none of their expectations were met.
- 49.8% reported that their most important expectation in the majority disability or pain improvement was met.
- 32.9% reported that their most important expectation was not met but others were.
The study further noted: “A large proportion of patients reported unfulfilled expectations of outcomes secondary to spine surgery, such as improvements in mental well-being. This may reflect unrealistic expectations that are ultimately unattainable and leading to patients’ dissatisfaction with surgery. It has also been shown that there is a large discrepancy between surgeons’ and patients’ expectation across different expectation dimensions.” However, “Despite this disparity, most patients (85%) were satisfied with the results of the surgery.”
An August 2022 study (17) investigated whether surgery met the patient’s preoperative expectations for back or leg pain or the achievement of minimum clinically important difference (MCID) on patient satisfaction following lumbar fusion.
- A total of 134 patients were included in this study. Patients demonstrated significant improvements in VAS back (0 – 10 pain scores) back and VAS leg (back and leg pain scores 0 – 10).
- At one year, 56.4% of patients had their VAS back expectations met compared with 59.5% for VAS leg.
- Similarly, at one year, 77.3% and 71.3% of patients achieved minimum clinically important difference for VAS back and leg, respectively.
The problems of opioids before surgery leading to greater risk
of failed back surgery syndrome and failure of spinal cord stimulators.
An August 2022 study (18) followed 96 people with chronic low back pain who were on long-term opioid therapy for their back-specific disability and health-related quality of life in patients with chronic low back pain. In surveying the people of this study, the researchers found these patients had worse back-specific disability, physical function, fatigue, limited participation in social settings, and pain interference outcomes. The researchers concluded: “The findings of this study are largely consistent with existing literature regarding the outcomes of long-term opioid therapy. Taken in conjunction with the well-established risks of opioid medications, these findings draw into question the utility of long-term opioid therapy for chronic low back pain.”
A November 2022 paper (19) examined opioid use for chronic pain prior to spinal surgery and the increased rate of post-operative adverse events in these patients. A subgroup of 2,112 patients using opioids preoperatively were followed. The researchers found “significantly higher incidence of infection compared to non-opioid users.”
Many patients choose to have spinal surgery because they do not want to spend a lifetime on painkillers or opioids. As these people wait for their surgery, many find themselves in need of more medications to get them to the surgery. This study from October 2020 (20) demonstrates how improper patient selection can lead to a medical disaster.
In this study, doctors wanted to know why spinal cord stimulation (SCS), while an an effective treatment in failed back surgery syndrome, may not work for everyone. Specifically people who were on opioids prior to the back surgery and the implantation of the spinal cord stimulator following failed back surgery.
- What they found was a higher preimplantation opioid doses associated with unsuccessful spinal cord stimulation suggesting the need for opioid tapering before implantation. With continuous SCS therapy and no explantation or revision due to inadequate pain relief, 39% of failed back surgery syndrome patients discontinued strong opioids, and 23% discontinued all opioids. This indicates that SCS should be considered before detrimental dose escalation.
In the above study the implication is that spinal cord stimulation could help decrease the need of painkillers. A February 2021 study found differently.(21) The authors suggested: “rigorous patient selection and pre-operative risk assessment for misuse and dependence are paramount to improving outcome after spinal cord stimulation implantation.”
The problems of diabetes in failed back surgery
An April 2024 study (22) of 552 patients who had spinal surgery, found: “diabetes significantly increases the risk of unsuccessful lumbar spine fusion outcome requiring revision surgery. Diabetes predisposes to the degeneration of adjacent spine segments and pseudoarthrosis at the fusion sites, and affects the structure of newly formed bone needed to stabilize fusion.”
A March 2024 study of 18,853 patients (2695 diabetic patients) (23) found: “Patients with diabetes had a significantly higher risk of developing complications after spinal fusion, particularly pulmonary and renal complications, in addition to surgical site infections and had a longer length of stay. These findings are important for informed discussions of surgical risks with patients and families before surgery.”
The problems of obesity in failed back surgery
A March 2024 study of 120 patients (24) assessed the outcomes of 63 patients considered obese and 57 patients considered overweight or less overweight. The researchers found patients with a Body Mass Index considered obese and patients with a Body Mass Index considered overweight or less, demonstrated comparable improvements for all spinopelvic radiographic measurements and patient reported outcomes. Patients considered obese demonstrated an increased incidence of cardiovascular complications, acute kidney injury, rod fractures, and reoperations when compared to patients who were not obese.
Does having an MRI to help diagnose failed back surgery syndrome help?
Should an MRI after surgery even be done?
A 2016 paper writes (25): “The treatment of chronic low back is difficult and is often ineffective. For treatment to be effective the cause of the pain has to be established but unfortunately in 80% to 95% of the patients the cause cannot be determined despite the existence of modern imaging techniques. . . . There exist no causal relationship between imaging findings of degenerated disc, lumbar facet arthritis, spondylosis, spondylolysis and spondylolisthesis, to the pain in these patients. Surgical treatment of non-specific back pain where no pathoanatomical diagnosis has been established is bound to fail. ”
A prepublication online December 2022 paper (26) writes: “Adequate treatment of failed back surgery syndrome is challenging, as its etiology is believed to be multifactorial and still not fully clarified. Accurate identification of the source of pain is difficult but pivotal to establish the most appropriate treatment strategy. Although the clinical utility of imaging in failed back surgery syndrome patients is still contentious, (debatable if having a post-surgical MRI is warranted, needed or even advised) objective parameters are highly warranted to map different phenotypes of failed back surgery syndrome and tailor each subsequent therapy. Although many imaging studies have been performed in failed back surgery syndrome patients, they are primarily focused on the preoperative setting or are not correlated with the patient’s symptoms in order to assess whether failed back surgery syndrome was indeed present and, if so, what imaging could have offered in failed back surgery syndrome patients specifically. Therefore, more evidence concerning imaging in failed back surgery syndrome patients is warranted, particularly for determining the source of pain and planning of follow-up treatment.”
Do doctors wait too long to ask the patient how they are doing after surgery?
Is this causing failed back surgery syndrome?
A March 2018 study (27) suggested their was too much variation in the follow up post-surgical period and this delay in follow up may be causing failed surgical outcomes. This may be why the numbers of failed back surgeries in the above study nearly doubled from six months post-op to one year post-op. In this paper, the researchers suggested that early postoperative results appeared to herald the longer term outcome. As such, a ‘wait and see policy’ in patients with a poor initial outcome at 3 months is not advocated.” Not reacting sooner to the apparent problems of the patient “could result in a failure to intervene early to achieve better long-term outcomes.”
Failure to return to work and physical activity
In an October 2020 paper (28) which wrote: “Studies have found that most patients are satisfied after spine surgery, with rates ranging from 53% to 90%. Patient satisfaction appears to be closely related to achieving clinical improvement in pain and disability after surgery. While the majority of the literature has focused on patients who report both satisfaction and clinical improvement in disability and pain, there remains an important subpopulation of patients who have clinically relevant improvement but report being dissatisfied with surgery.” The researchers then asked why were the patient’s dissatisfied? They found: “Several modifiable factors, including psychological distress, current smoking status, and failure to return to work and physical activity, helped explain why patients report being dissatisfied with surgery despite clinical improvement in disability or pain.”
Some people will get benefit eventually from surgery. Some will not. Doctors, including those from the University of Bern in Switzerland published their research findings (29) on patients who had to undergo multiple spinal surgeries. When they examined patients 12 months after their last surgery they found that the more surgeries a patient had, the less likely they would have clinical success. The Swiss doctors warned that when suggesting to patients further spinal surgeries, the patients needed to be advised that the outcome may not be good and that they, the patient, should set realistic expectations so as not to be discouraged by poor surgical outcomes.
“A number of controversial issues concerning the management of
failed back surgery syndrome are regularly debated. . . “
In a July 2019 (30) paper, spinal surgeons and neurosurgeons tried to come up with a program to help people with Failed Back Surgery Syndrome. They wrote: “A number of controversial issues concerning the management of failed back surgery syndrome are regularly debated, but no clear consensus has been reached. (On how to treat it). . . “Failed back surgery syndrome results from a cascade of medical and surgical events that have led to and left the patient with chronic back and radicular pain. This pain often remains refractory to sporadic management strategies for a considerable proportion of these patients. . . “
An August 2022 paper (31) noted: “The most common reasons for early reoperation and late operation were surgical site infection and adjacent segment diseases, respectively. Osteoporosis and diabetes were independent risk factors for early reoperation, and multilevel fusion was independent risk factor for late reoperation. ”
Pain and fear of movement following spinal surgery
Let’s look at two studies, seven years apart, from the same learning institute. The research concerns pain and fear of movement following spinal surgery and which patients would be at greater risk for poorer recovery.
From 2011: Patients with back pain have many concerns and fears when it comes to being able to move pain-free. Surgery is supposed to take care of this fear. Researchers from the University of Gothenburg, Sweden (32) followed 97 patients after their spinal disc surgery looking for a post-surgical occurrence of kinesiophobia “fear of movement,” a tell-tale sign of unsuccessful back surgery. What they found was surprising.
- Half of the patients suffered from kinesiophobia 10-34 months after surgery for disc herniation.
- Prior to surgery these patients were already classified as more disabled, had more pain, more catastrophizing thoughts, more symptoms of depression, lower self-efficacy, and poorer health-related quality of life than patients.”
For many whom surgery would seemingly be most helpful, the surgery itself did not reverse their problems and made their fear of extremely painful movement worse
Seven years later, 2018. A different team of researchers from the University of Gothenburg, Sweden (33) recruited a study in 2016 which they hoped would help patients following spinal surgery with problems of health-related quality of life, back and leg pain intensity, pain catastrophizing, kinesiophobia, depression, and anxiety. In 2018 they published their findings:
“A high proportion of the patients did not reach the WHO (World Health Organization) recommendations on physical activity and are therefore at risk of poor health due to insufficient physical activity. We also found a negative association between both fear of movement and disability, and the number of steps per day. Action needs to be taken to motivate patients to be more physically active before surgery, to improve health postoperatively. There is a need for interventions aimed at increasing physical activity levels and reducing barriers to physical activity in the prehabilitation phase of this patient group.”
In November 2019, (34) another study confirmed these findings:
“Depression and fear of movement were more important predictors of the execution of activities of daily living and participation in social life compared to morphological (internal structure damage) markers. Elevated depressive symptoms and fear of movement might indicate limited adaptation and coping regarding the disease and its consequences.”
A May 2024 study (35) assessed the appropriateness of surgical decisions in degenerative spondylolisthesis. The authors write: “Selecting patients with lumbar degenerative spondylolisthesis for surgery is difficult. Appropriate use criteria (the research and evidence based decision process in sending a patient or not sending a patient to surgery) have been developed to clarify the indications for lumbar degenerative spondylolisthesis surgery.” The appropriate use criteria however as a tool to understand the appropriateness of surgery in these patients was not able to identify which patients had a greater treatment effect of surgery when compared to non-surgical care. The benefit of surgery relative to non-surgical care was not significantly greater. However, better surgical outcomes were seen in more severe cases.
A heightened sense of pain from an altered pain processing center
A November 2022 study (36) examined the problem of altered central pain processing in failed back surgery syndrome patients. Altered central pain processing sounds exactly as to what is is. You have an altered sense of pain (worse pain than you should) and it is coming from the central nervous system. In this study, the researchers found that the 34 patients diagnosed with failed back surgery syndrome were more sensitive to pressure sensation and a conditioned pain modulation. The doctors tested the patients with a pain stimulus. While the pain stimulus was not increased, over time the patient felt more pain from the same stimulus.
Conservative care treatments
Pharmaceutical
A May 2022 update in STATPEARLS, (37) a book of the National Library of Medicine writes: “Studies of conservative treatment specifically for failed back surgery syndrome are rare, and the studies that do exist are often contradictory. Common pharmacologic treatments include non-steroidal anti-inflammatory drugs (NSAIDs), opioids, anticonvulsants, and antidepressants. NSAIDs are commonly prescribed drugs for many different etiologies of lower back pain, for which they have been shown to have an advantage over placebo. While opioids are commonly used to treat chronic pain, evidence for their use in FBSS is generally weak, and the risk of dependence and resultant substance use disorder must be strong consideration before their use.
Because there was little long-term data on Spinal cord stimulation in helping patients with failed back surgery syndrome, doctors conducted patient reviews in people who had spinal cord stimulation devices, some for 20 years or more. In this May 2022 study (38), researchers looked at overall patient satisfaction, pain intensity, and adverse events for 191 patients who received a permanent SCS implant. Secondary health measures included the influence of opioid and nicotine use on pain reduction after therapy.
- 78.5% of the patients were satisfied with the treatment outcome, with a significant pain reduction of an average three points on a Numeric Rating Scale (0-10).
- Opioid and nicotine usage did not have a significant link with the pain reduction one year after the treatment.
- Devices had an average battery lifespan of 8.4 years. A total of 248 revisions were recorded. A total of 24 patients (11.7%) acquired an infection; 7 of 204 patients had an infection during the trial period, 2 of 191 patients had an infection in the first postoperative year, and 15 of 191 patients had an infection after the first year. The average time to infection, if not in the first year, was 10.1 years.
Conclusions: “A successful long-term outcome regarding pain relief in patients with predominant radicular pain due to FBSS is established with SCS therapy.”
In this paper doctors at John Hopkins University wrote:
“Spinal cord stimulation (SCS) has been considered as an alternative therapy to reduce opioid requirements in certain chronic pain disorders. However, information on long-term opioid consumption patterns and their impact on Spinal cord stimulation device explantation is lacking.
(The researchers) conducted a retrospective study of 45 patients to characterize long-term patterns of opioid usage after Spinal cord stimulation implantation.
Results:
- Daily morphine equivalent dosage increased in 40% of patients
- Daily morphine equivalent dosage decreased in 40% of patients
- and 20% of patients used the same amount of pain medications at 1-year follow-up
Spinal cord stimulation removed because of failure – when the spinal cord stimulators were removed – pain medication usage dropped in some patients
- Twelve (27%) underwent explantation due to treatment failure at a median of 18 months after implantation.
- Following explantation, reduction in the daily medication was seen in 92% of patients with dosages falling below pre-operative baseline in nine.
- (The) results indicate that daily opioid consumption does not decrease in most patients one-year after Spinal cord stimulation implantation.
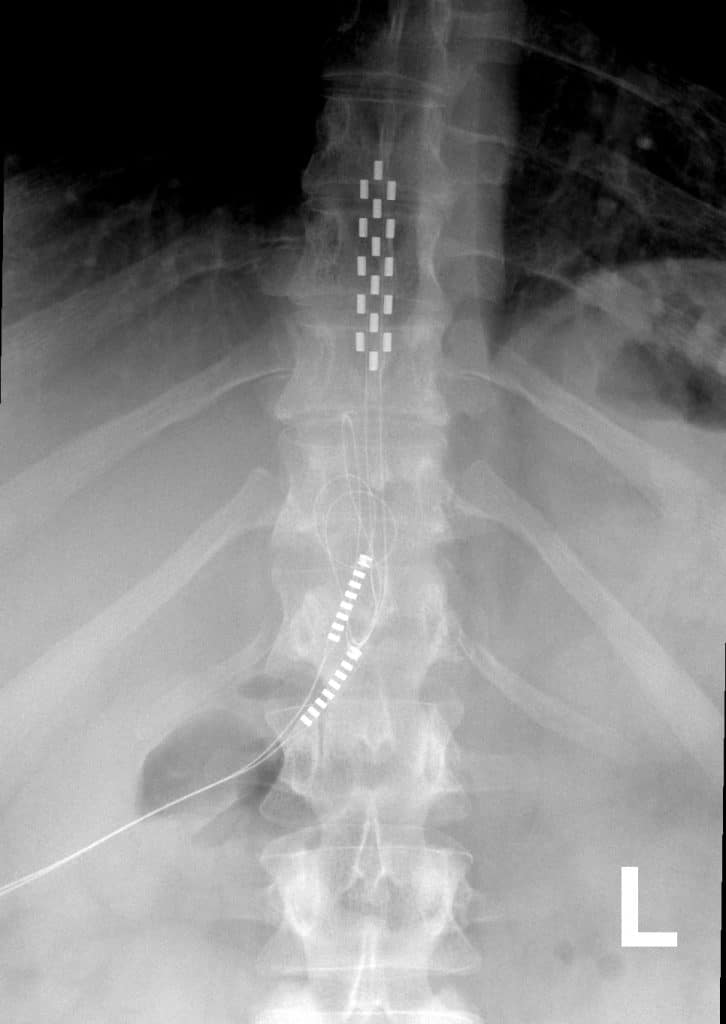
Anterior view X-ray of a Medtronic Spinal Cord Stimulator (SCS) with 5-6-5 paddle lead implanted in the posterior epidural space of the thoracic spine. Image used in compliance with Wikimedia Commons attribution: Mconnell, CC BY 3.0, via Wikimedia Commons
{kind=link}
Research demonstrates that current SCS technology does not reliably help a larger number of patients reduce opioid usage
A January 2020 report in the journal Neuromodulation (39) agrees:
“With only half of chronic opioid users demonstrating meaningful opioid reduction after SCS implantation, we demonstrate that current SCS technology does not reliably help a larger number of patients reduce opioid usage. Women, older age, and preoperative MED (pain medication usage) are predictive of meaningful opioid reduction but only one of these is modifiable. As not all patients saw benefit from their therapies, there is still much room for improvement in the treatment of refractory chronic pain that is associated with failed back surgery syndrome and chronic regional pain syndrome.”
Lumbar sympathetic ganglion block
A January 2023 study (40) compared pain and quality of life in patients with failed back surgery syndrome who responded and did not respond to Lumbar sympathetic ganglion block. Lumbar sympathetic ganglion block reduced pain at all-time points. Patients who showed more than 50% reduction in pain at one week had improved quality of life simultaneously. However, patients who showed less than 50% reduction in pain at one week had no improvement in quality of life. Lumbar sympathetic ganglion block did not influence the coldness of the leg.
Ab September 2024 study (42) suggests: “Pulsed radiofrequency, adhesiolysis (scar tissue removal) and spinal cord stimulators have a higher level of evidence with a high safety margin and should be considered as interventional treatment options when conservative treatment fails.
Regenerative medicine injections
There is not much by way of research on any conservative care options much less regenerative medicine. This is pointed out in a May 2023 updated in the medical publication Stat Pearls (41) :
“Therapies for the treatment of failed back surgery syndrome broadly split into conservative (physical therapy or medication) and aggressive (interventional or surgical) management. Conservative management should always be the first option before invasive techniques in patients without indications for emergency surgery.
Studies of conservative treatment specifically for failed back surgery syndrome are rare, and the studies that do exist are often contradictory. Common pharmacologic treatments include non-steroidal anti-inflammatory drugs (NSAIDs), opioids, anticonvulsants, and antidepressants. NSAIDs are commonly prescribed drugs for many different etiologies of lower back pain, for which they have been shown to have an advantage over placebo. While opioids are commonly used to treat chronic pain, evidence for their use in failed back surgery syndrome is generally weak, and the risk of dependence and resultant substance use disorder must be strong consideration before their use. As such these should be considered a treatment of last resort and undertaken in a multidisciplinary program. Small trials using anticonvulsants such as gabapentinoids or antidepressants in FBSS therapy have shown promising initial results, but long-term efficacy is undetermined.”
They key to this 2023 updated on failed back surgery is that the little research there is, does not include much on regenerative medicine.
There has to be a realistic expectation of what regenerative medicine can do and what they can’t do. If there are issues of continued pain following a fusion surgery, regenerative medicine may be effective in helping pain if there are issues with ligament and tendon instability causing segmental disease above and below the fusion. Regenerative medicine may help strengthen the tendon/muscle attachments and help patients who suffer from continued spasms. In situations where a laminectomy was performed, exploring the spinal ligaments as a possible cause of instability and pain may be considered.
Contact us and related articles
If you have chronic back pain, have had painkillers, physical therapy, and other conservative care options that have not helped, and, now you are being told to have surgery. We may be able to help reduce pain and increase function.
Regenerative medicine injections may be an alternative for you. Many people benefit from these treatments, but, they do not work for everyone. Will it work for you? Get a FREE phone consultation.
Call for a free phone consultation with our staff.
800-300-9300 or 310-231-7000 or email
Related articles:
Pain after spinal fusion may be from post-surgical muscle damage
Lumbar spinal stenosis – surgery and injections | Joint Rehab Los Angeles
References:
1 Yeo J. Failed back surgery syndrome-terminology, etiology, prevention, evaluation, and management: a narrative review. Journal of Yeungnam medical science.
2 Alizadeh R, Sharifzadeh SR. Pathogenesis, etiology and treatment of failed back surgery syndrome. Neurochirurgie. 2021 Sep 17.
3 Martin BI, Mirza SK, Comstock BA, Gray DT, Kreuter W, Deyo RA. Are lumbar spine reoperation rates falling with greater use of fusion surgery and new surgical technology? Spine 2007 Sep 1;32(19):2119-26.
4 Deyo RA, Martin BI, Kreuter W, Jarvik JG, Angier H, Mirza SK . Revision surgery following operations for lumbar stenosis J Bone Joint Surg Am. 2011 Nov 2;93(21):1979-86.
5 Amirdelfan K, Webster L, Poree L, Sukul V, McRoberts P. Treatment options for failed back surgery syndrome patients with refractory chronic pain: an evidence based approach. Spine. 2017 Jul 15;42(1):S41-52.
6 Jung JM, Chung CK, Kim CH, Choi Y, Kim MJ, Yim D, Yang SH, Lee CH, Hwang SH, Kim DH, Yoon JH. The Long-Term Reoperation Rate Following Surgery for Lumbar Stenosis: A Nationwide Sample Cohort Study with a 10-Year Follow-Up. Spine. 2020 Apr 24.
7 Stanton EW, Chang KE, Formanek B, Buser Z, Wang J. The incidence of failed back surgery syndrome varies between clinical setting and procedure type. Journal of Clinical Neuroscience. 2022 Sep 1;103:56-61.
8 Wang SK, Wang P, Li XY, Kong C, Niu JY, Lu SB. Incidence and risk factors for early and late reoperation following lumbar fusion surgery. Journal of Orthopaedic Surgery and Research. 2022 Dec;17(1):1-9.
9 van Hooff ML, van Dongen JM, Coupé VM, Spruit M, Ostelo RW, de Kleuver M. Can patient-reported profiles avoid unnecessary referral to a spine surgeon? An observational study to further develop the Nijmegen Decision Tool for Chronic Low Back Pain. PloS one. 2018 Sep 19;13(9):e0203518.
10 Oliveira RB, Oliveira IO, Antonioli E, Lenza M, Ferretti M. Clinical outcome analysis in surgical patients enrolled in a Second Opinion Program in spine surgery. Einstein (São Paulo). 2022 Apr 1;20.
11 Mathieu J, Robert MÈ, Châtillon CÉ, Descarreaux M, Marchand AA. Appropriateness of specialized care referrals for LBP: a cross-sectional analysis. Frontiers in Medicine. 2023;10.
12 Mancuso CA, Reid MC, Duculan R, Girardi FP. Improvement in Pain after Lumbar Spine Surgery: The Role of Preoperative Expectations of Pain Relief. Clin J Pain. 2016 Mar 28.
13. Calpin P, Imran A, Harmon D. A Comparison of Expectations of Physicians and Patients with Chronic Pain for Pain Clinic Visits. Pain Pract. 2016 Mar 15. doi: 10.1111/papr.12428.
14 Rabah NM, Khan HA, Levin JM, Winkelman RD, Mroz TE, Steinmetz MP. The association between patient rating of their spine surgeon and quality of postoperative outcome. Journal of Neurosurgery: Spine. 2020 Dec 18;34(3):449-55.
15 Alhaug OK, Dolatowski FC, Solberg TK, Lønne G. Predictors for failure after surgery for lumbar spinal stenosis, a prospective. The Spine Journal. 2022 Nov 5.
16 Rampersaud YR, Canizares M, Perruccio AV, Abraham E, Bailey CS, Christie SD, Evaniew N, Finkelstein JA, Glennie RA, Johnson MG, Nataraj A. Fulfillment of Patient Expectations After Spine Surgery is Critical to Patient Satisfaction: A Cohort Study of Spine Surgery Patients. Neurosurgery.
17 Cha ED, Lynch CP, Jadczak CN, Mohan S, Geoghegan CE, Singh K. Meeting Patient Expectations or Achieving a Minimum Clinically Important Difference: Predictors of Satisfaction Among Lumbar Fusion Patients. Asian Spine Journal. 2021 Sep 2.
18 Schultz MJ, Licciardone JC. The effect of long-term opioid use on back-specific disability and health-related quality of life in patients with chronic low back pain. Journal of Osteopathic Medicine. 2022 Aug 11.
19 Gonzalez GA, Corso K, Miao J, Rajappan SK, Porto G, Anandan M, O’Leary M, Wainwright J, Smit R, Hines K, Franco D. Does pre-operative opiate choice increase risk of post-operative infection and subsequent surgery?. World Neurosurgery. 2022 Nov 14.
20 Nissen M, Ikäheimo TM, Huttunen J, Leinonen V, Jyrkkänen HK, von und zu Fraunberg M. Higher Preimplantation Opioid Doses Associated With Long‐Term Spinal Cord Stimulation Failure in 211 Patients With Failed Back Surgery Syndrome. Neuromodulation: Technology at the Neural Interface.
21 Hwang BY, Negoita S, Duy PQ, Tesay Y, Anderson WS. Opioid use and spinal cord stimulation therapy: the long game. Journal of Clinical Neuroscience. 2021 Feb 1;84:50-2.
22 Wilson C, Czernik PJ, Elgafy H, Khuder S, Serdahely K, Rowland A, Lecka-Czernik B. Diabetes increases risk of lumbar spinal fusion complications; association with altered structure of newly formed bone at the fusion site. JBMR Plus. 2024 Apr 15:ziae053.
23 Ruggiero N, Soliman MA, Kuo CC, Aguirre AO, Quiceno E, Saleh J, Yeung K, Khan A, Hess RM, Lim J, Smolar DE. The Effect of Diabetes on Complications After Spinal Fusion: A Systematic Review and Meta-Analysis. World neurosurgery.:S1878-8750.
24 Marquardt MD, Gibbs D, Grossbach A, Keister A, Munjal V, Moranville R, Mallory N, Toop N, Dhaliwal J, Marquardt H, Xu D. Impact of obesity on adult spinal deformity (ASD) long-segment spinal fusion radiographic and clinical outcomes. Clinical Neurology and Neurosurgery. 2024 Feb 21:108187.
25 Dhillon KS. Spinal fusion for chronic low back pain: a ‘Magic Bullet’or Wishful Thinking?. Malaysian orthopaedic journal. 2016 Mar;10(1):61.
26 Witkam RL, Buckens CF, van Goethem JW, Vissers KC, Henssen DJ. The current role and future directions of imaging in failed back surgery syndrome patients: an educational review. Insights into Imaging. 2022 Dec;13(1):1-5.
27 Fekete TF, Loibl M, Jeszenszky D, Haschtmann D, Banczerowski P, Kleinstück FS, Becker HJ, Porchet F, Mannion AF. How does patient-rated outcome change over time following the surgical treatment of degenerative disorders of the thoracolumbar spine?. European spine journal. 2018 Mar;27(3):700-8.
28 Sivaganesan A, Khan I, Pennings JS, Roth SG, Nolan ER, Oleisky ER, Asher AL, Bydon M, Devin CJ, Archer KR. Why are patients dissatisfied after spine surgery when improvements in disability and pain are clinically meaningful?. The Spine Journal. 2020 Oct 1;20(10):1535-43.
29 Zehnder P, Aghayev E, Fekete TF, Haschtmann D, Pigott T, Mannion AF. Influence of previous surgery on patient-rated outcome after surgery for degenerative disorders of the lumbar spine. Eur Spine J. 2016 Aug;25(8):2553-62.
30 Gatzinsky K, Eldabe S, Deneuville JP, Duyvendak W, Naiditch N, Van Buyten JP, Rigoard P. Optimizing the Management and Outcomes of Failed Back Surgery Syndrome: A Proposal of a Standardized Multidisciplinary Team Care Pathway. Pain Res Manag. 2019 Jul 8;2019:8184592. doi: 10.1155/2019/8184592. PMID: 31360272; PMCID: PMC6644221.
31 Wang SK, Wang P, Li XY, Kong C, Niu JY, Lu SB. Incidence and risk factors for early and late reoperation following lumbar fusion surgery. Journal of Orthopaedic Surgery and Research. 2022 Dec;17(1):1-9.
32. Svensson GL, Lundberg M, Östgaard HC, Wendt GK. High degree of kinesiophobia after lumbar disc herniation surgery: A cross-sectional study of 84 patients. Acta orthopaedica. 2011 Dec 1;82(6):732-6.
33 Lotzke H, Jakobsson M, Gutke A, Hagströmer M, Brisby H, Hägg O, Smeets R, Lundberg M. Patients with severe low back pain exhibit a low level of physical activity before lumbar fusion surgery: a cross-sectional study. BMC musculoskeletal disorders. 2018 Dec;19(1):1-9.
34 Quack V, Boecker M, Mueller CA, Mainz V, Geiger M, Heinemann AW, Betsch M, El Mansy Y. Psychological factors outmatched morphological markers in predicting limitations in activities of daily living and participation in patients with lumbar stenosis. BMC musculoskeletal disorders. 2019 Dec;20(1):1-9.
35 Mannion AF, Mariaux F, Werth PM, Pearson AM, Lurie JD, Fekete TF, Kohler M, Haschtmann D, Kleinstueck FS, Jeszenszky D, Loibl M. Evaluation of “appropriate use criteria” for surgical decision-making in lumbar degenerative spondylolisthesis. A controlled, multicentre, prospective observational study. European Spine Journal. 2024 Feb 28:1-3.
36 Nie C, Chen K, Chen J, Zhu Y, Jiang J, Jin X, Xia X, Zheng C. Altered central pain processing assessed by quantitative sensory testing in patients with failed back surgery syndrome. Neurophysiologie Clinique. 2022 Nov 1;52(6):427-35.
37 Orhurhu VJ, Chu R, Gill J. Failed Back Surgery Syndrome. [Updated 2022 May 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-.
38 Puylaert M, Nijs L, Buyse K, Vissers K, Vanelderen P, Nagels M, Daenekindt T, Weyns F, Mesotten D, Van Zundert J, Van Boxem K. Long-Term Outcome in Patients With Spinal Cord Stimulation for Failed Back Surgery Syndrome: A 20-Year Audit of a Single Center. Neuromodulation: Technology at the Neural Interface. 2022 May 14.
39 Dougherty MC, Woodroffe RW, Wilson S, Gillies GT, Howard III MA, Carnahan RM. Predictors of reduced opioid use with spinal cord stimulation in patients with chronic opioid use. Neuromodulation: Technology at the Neural Interface. 2020 Jan;23(1):126-32.
40 Lee JY, Sim WS, Kim J, Yang S, Ro H, Kim CJ, Kim SU, Park HJ. The analgesic effect of lumbar sympathetic ganglion block in patients with failed back surgery syndrome. Frontiers in Medicine. 2022;9.
41 Orhurhu VJ, Chu R, Gill J. Failed Back Surgery Syndrome. [Updated 2021 May 12]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK539777/
42 van de Minkelis J, Peene L, Cohen SP, Staats P, Al-Kaisy A, Van Boxem K, Kallewaard JW, Van Zundert J. 6. Persistent spinal pain syndrome type 2. Pain Pract. 2024 Sep;24(7):919-936.
.