






Marc Darrow, MD, JD.
Most people with shoulder pain directly attributed to tennis will suggest that it was “this one serve,” or “this one return serve,” that was the point of their injury. Then after further talking they will reveal that their shoulder has actually been the cause of on and off discomfort for some time at that this “acute” injury was the accumulation of a lot of wear and tear.
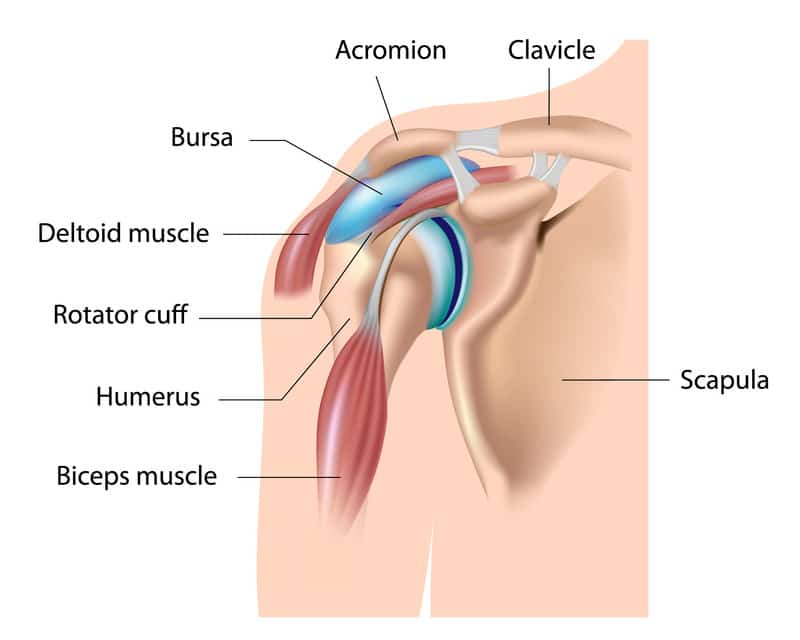
On examination, a weekend warrior or semi-pro or pro tennis player can show shoulder impingement problems, superior labral (SLAP) tears, rotator cuff tears and acromioclavicular joint pain.
A problem of a tennis shoulder can go further than just the shoulder. It can go into the spine and the elbow. This is not a new discovery. A paper (1) was published in the American Journal of Sports Medicine describing tennis shoulder as more than just a shoulder pain but as a chronic problem that could eventually lead to spine problems. This is what those researchers of nearly 50 years ago wrote: “(A) depression (droopy, slopped) of the exercised shoulder was found in skilled tennis players, and in other athletes employing the overhand motion. The deformity is attributed to stretching of the shoulder elevating muscles and hypertrophy of the extremity. Most symptoms were over the anterior (front) rotator cuff, and occurred on abduction of the arm. Shoulder depression results in a relative abduction and abduction causes impingement of the cuff. Shoulder droop may induce thoracic outlet syndrome and may simulate scoliosis in the athlete.”
Forty-four years later, an October 2020 paper (2) extended the list of problems that shoulder injuries could play part in and extended these problems to that of the elbow and wrist: “Common injuries include internal shoulder impingement, rotator cuff pathology, shoulder labral tears, elbow tendinopathies, as well as extensor carpi ulnaris tendinopathies and subluxation, problems in the wrist). Posterior shoulder instability, distal humeral bone stress (at the elbow), elbow medial collateral ligament, and nondominant wrist ulnar collateral ligament injuries are not commonly reported injuries, but they are of significant clinical importance (in tennis players).
A point that should be made here is that for some people their shoulder problems are much more advanced than simple treatments can help.
Over the years I have seen many athletes who have shoulder problems. For most of these athletes, their problems were that of the rotator cuff, the previously mentioned problems of impingement and unfortunately a lot of shoulder pain. For some, their shoulder pain extended into their neck. For others the problems of a droopy shoulder or one shoulder lower than the other was causing them significant back problems. But the problems can go even further.
Backhands, backhand volleys, and the follow-through phase of forehands and serves

A June 2023 study (5) looked at the problem of micro-traumatic posterior shoulder instability in tennis players. A problem the study authors say “can be the result of repetitive microtrauma in combinations of shoulder flexion, horizontal adduction, and internal rotation, which are characteristic shoulder positions for backhands, backhand volleys, and the follow-through phase of forehands and serves.”
In treating this problem the authors write: “Initial management of micro-traumatic posterior shoulder instability typically involves rehabilitation focusing on posterior rotator cuff and deltoid function and eventually progressing exercises into the sagittal and horizontal adduction plane. Due to the large demands placed on the shoulder in tennis, some individuals may require surgery if they fail appropriate evidence-based conservative management.”
A challenge the authors noted was the lack of medical research on what was the best evidence-based conservative management. Let’s review some of the research below.
Treatment for Tennis Shoulder Injuries
Activity Modification
A top treatment for tennis shoulder is also one of the most unpopular treatments. The treatment is called Activity Modification. Activity Modification simply means that you have stopped playing tennis or you are playing less frequently. Many people do try resting the shoulder. For many people this works very well and they are able to resume playing at their previous levels. For other however, rest was “only a waste of time.” As soon as these people felt that they have rested their shoulder long enough, they returned to the court. Once they did they found that the pain came back immediately or soon after they resumed playing. They were back to square one.
Non-steroidal Anti-inflammatory Medications (NSAIDs)
For many people NSAIDs can make their shoulders feel better in the short-term. However, higher doses maybe needed in the long-term to achieve similar results. In a September 2019 study (3) doctors compared ibuprofen and acetaminophen in patients with shoulder pain. In both groups (ibuprofen and acetaminophen), there was significant variability in response to these medications. Even if the average pain score was improved, several patients exhibited worsening of their condition. . .However, the answer to the question of which medication provided more benefit to the patients remained elusive. Ibuprofen appeared to treat the issues related directly to the perception of pain and, consequently, the function of upper extremities better, whereas acetaminophen administration resulted in better indices for Quality of Life.
Physical Therapy
People who play tennis are frequently diagnosed with rotator cuff tendinopathy. I frequently see patients with an MRI of a shoulder tendon tear or an MRI of a problem of chronic tendinopathy. Tendinopathy is a more recent term to describe a chronic pathology of a tendon that causes shoulder pain. The problem of Tendinopathy can be divided into two broad categories:
- Tendinitis means inflammation of the shoulder tendons. This is the characteristic swelling that comes with a worsening wear and tear or acute injury.
- Tendinosis is the “old, nagging injury.” The tendon is injured but the body has given up trying to heal it. It is an injury without inflammation. Why did the body give up? In some of the people we see, it comes as the result of a long and extensive anti-inflammatory or cortisone treatment history.
Many people have had successful physical therapy for treating rotator cuff tendinitis, tendinosis, and shoulder impingement syndrome. The idea of course being the avoidance of movement that causes pain and postural adjustments in the workplace setting to help avoid having the shoulders roll in or sloop.
Physical therapy may be less effective or not work at all in situations where the shoulder tendons are stretched or damaged enough that they cannot provide the resistance needed to strengthen the muscles.
Tennis Shoulder Tendinopathy and Shoulder Impingement Treatment
For most, shoulder impingement means pain in the front of you shoulder. Many people continue to play tennis through their pain. They complain about pain at the top of their shoulder, the side of their shoulder and when they extended their hands over their head during the serve. If you have chronic shoulder pain affecting your game you have probably tried remedies and exercises listed above including RICE (rest, ice, compression, and elevation) and self-medicating with anti-inflammatory medications that may have helped short-term, but did not help you play long-term.
When you got to the point where you may have to stop playing, this is when you decided to get medical care. Medical care may not have been to your likening. You may have not liked the suggest your doctor gave you to stop playing for a while to see if your shoulder heals on its own. You may have liked it worse when after a long bout of rest, you picked up a racquet and the same pain remained.
When you returned to your doctor after the rest period and want to try something else to help accelerate your healing, as mentioned above, you may have been told to go to physical therapy to see if that works. You can also try a cortisone injection.
Muscle atrophy in the infraspinous fossa of the dominant arm of overhead athletes
Basic anatomy tells us that tendons attach muscles to bones. When that muscle is atrophied it is either from overuse or the tendon is damaged and not providing sufficient strength for the muscle to be able to contract. When the muscle cannot contract, pull or push against the bone, the muscle atrophies.
An October 2020 study (4) looked at 153 male professional tennis players. The tennis players underwent a musculoskeletal screening examination that included visual inspection of the infraspinous muscle. The muscle illustrated above. What these doctors were saying is that many tennis player have a visually observable atrophy in the serving arm and the tennis players may not be aware of it. These were the findings:
- In the 153 players, dominant-arm infraspinatus atrophy was observed in 92 players (60.1%).
- Visually observed infraspinatus muscle atrophy is a common finding in the dominant shoulder of asymptomatic male professional tennis players and is significantly correlated with external rotation weakness.
- This condition is present in uninjured players without known shoulder pathology and is not related to glenohumeral joint internal rotation, total rotation range of motion, or scapular dysfunction. Players with visually observed infraspinatus atrophy should be evaluated for external rotation strength and may require preventive strengthening.
What should be pointed out is that the muscle is atrophying and in many cases it is atrophying to prevent future injury or because it is already injured.
In our research which appears in the peer-reviewed journal Cogent Medicine. The study can be found here in its entirety: Treatment of shoulder osteoarthritis and rotator cuff tears with bone marrow concentrate and whole bone marrow injections with a June 20, 2019 publication date.
Here we suggested:
- Patients with rotator cuff tendinopathy and degenerative shoulder disease would benefit from either one and two treatments. Patients reported significant improvements in resting pain, active pain, and functionality score when compared to baseline.
- These groups also experienced a 42.25% and 50.17% overall improvement respectively.
- The group that received two treatments experienced statistically significant improvements in active pain when compared to the group that received one injection.
- There were no significant outcome differences between rotator cuff tear and osteoarthritis patients.
Conclusions: Our study demonstrated that patients diagnosed with shoulder osteoarthritis or rotator cuff tears experienced symptomatic improvements in pain and functionality when injected with bone marrow concentrate (BMC) or whole bone marrow (WBM). Further randomized control studies are needed to validate these findings.
1 Martin C, Sorel A, Touzard P, Bideau B, Gaborit R, DeGroot H, Kulpa R. Influence of the forehand stance on knee biomechanics: Implications for potential injury risks in tennis players. Journal of sports sciences. 2020 Dec 7:1-9.
2 Martin C, Sorel A, Touzard P, Bideau B, Gaborit R, Degroot H, Kulpa R. Can the Open Stance Forehand Increase the Risk of Hip Injuries in Tennis Players?. Orthopaedic Journal of Sports Medicine. 2020 Dec 11;8(12):2325967120966297.
1431
Stem Cell Therapy is the injection of a damaged area of the body with stem cells that have been drawn from the patient’s own bone marrow. Stem cells are “de-differentiated pluripotent” cells, which mean that they continue to divide to create more stem cells; these cells eventually “morph” into the tissue needing repair—for our purposes, collagen, bone, and cartilage.
The excitement in the medical community is focused on how stem cells work, rebuilding the damaged part of the body from within by turning a diseased joint environment into a healing joint environment.
This is research published in the Orthopaedic journal of sports medicine.(9).
“Cell-based therapies and regenerative medicine offer safe and potentially efficacious treatment for sports-related musculoskeletal injuries. Basic science and preclinical studies that support the possibility of enhanced recovery from sports injuries using cell-based therapies are accumulating. . . ”
In the Journal of Knee Surgery (10) doctors from the Department of Orthopaedic Surgery, University of Pittsburgh had this to say:
- “Biologic agents (stem cells and blood platelets or PRP therapy) are gaining popularity in the management of bon and soft tissue conditions about the knee. They are becoming the mainstay of nonoperative therapy in the high-demand athletic population. . . . Studies assessing the utility of stem cells have shown encouraging results in the setting of osteoarthritis. “As the volume and quality of evidence continue to grow, biologic agents are poised to become an integral component of comprehensive patient care throughout all orthopedic specialties.”
PRP therapy treatments involve collecting a small amount of your blood and spinning it in a centrifuge to separate the platelets from the red cells. The collected platelets are then injected back into the injured area to stimulate healing and regeneration.
Doctors at the Mayo Clinic published research on ultrasound guided platelet rich plasma injections for treatment of symptoms associated with acetabular hip labral tears. What the Mayo Clinic researchers hoped to answer was whether PRP was safe and effective. The results were published in the American journal of physical medicine & rehabilitation.(9)
- The researchers looked at 8 patients who have previously failed conservative management and received ultrasound-guided injection of PRP at the site of hip labrum tear. The patients were assessed for pain and functionality at the start of treatment, then 2, 6, and 8 weeks after injection.
- The findings: Results were good, improvements in pain and function were seen at the 2, 6 and 8 week marks post injection.
- The conclusion: “Ultrasound-guided injection of PRP holds promise as an emerging, minimally-invasive technique toward symptom relief, reducing pain, and improving function in patients with hip labral tears.”
In our own clinical observations, we have seen good results using stem cell injections to help repair varying degrees of hip labrum injuries. We currently use bone marrow derived stem cells which are taken from the patient and reinjected into the hip labrum area. The decision as to which of these treatments to used is made at the time of the physical examination and a determination is made that the patient is a good candidate for treatment and should have a realistic expectation of treatment success.
Call for a free phone consultation with our staff 800-300-9300
Similar articles:
References
1. Priest JD, Nagel DA. Tennis shoulder. The American journal of sports medicine. 1976 Jan 1;4(1):28-42.
2. Shannon N, Cable B, Wood T, Kelly IV J. Common and Less Well-known Upper-limb Injuries in Elite Tennis Players. Current sports medicine reports. 2020 Oct 1;19(10):414-21.
3. AlRuthia Y, Alghadeer S, Balkhi B, Almalag HM, Alsobayel H, Alodaibi F, Alayoubi F, Alkhamali AS, Alshuwairikh S, Alqahtani FN, Alsanawi H. Efficacy of acetaminophen versus ibuprofen for the management of rotator cuff-related shoulder pain: Randomized open-label study. Saudi Pharmaceutical Journal. 2019 Sep 1;27(6):882-8.
4 Ellenbecker TS, Dines DM, Renstrom PA, Windler GS. Visual observation of apparent infraspinatus muscle atrophy in male professional tennis players. Orthopaedic Journal of Sports Medicine. 2020 Oct 27;8(10):2325967120958834.
5 Watson L, Hoy G, Wood T, Pizzari T, Balster S, Barwood S, Warby SA. Posterior Shoulder Instability in Tennis Players: Aetiology, Classification, Assessment and Management. International Journal of Sports Physical Therapy. 2023 Jun 1;18(3):769-88.
1 Martin C, Sorel A, Touzard P, Bideau B, Gaborit R, DeGroot H, Kulpa R. Influence of the forehand stance on knee biomechanics: Implications for potential injury risks in tennis players. Journal of sports sciences. 2020 Dec 7:1-9.
2 Martin C, Sorel A, Touzard P, Bideau B, Gaborit R, Degroot H, Kulpa R. Can the Open Stance Forehand Increase the Risk of Hip Injuries in Tennis Players?. Orthopaedic Journal of Sports Medicine. 2020 Dec 11;8(12):2325967120966297.
1431