






Platelet Rich Plasma Therapy or sometimes referred to as PRP is a regenerative / biologic therapy that uses the healing factors of your blood to rebuild and repair damaged tissue. Doctors have been using this treatment for many years because PRP can be seen as an alterative to cortisone injection and surgical intervention.
In the research below we will see doctors use the term “orthobiologic” in describing PRP treatments. Orthobiologic means that a treatment is used that is derived from living cells from within your own body. The treatment is designed to accelerate healing, specifically in soft tissue such as ligaments, tendons, muscles and bones. We have employed this treatment at our Los Angeles office for many years.
PRP treatments are derived from you. We collect a small amount of your blood, similar to the blood taken for standard blood work, and then take it over to a centrifuge where the blood is spun. The spinning helps separate out the blood’s platelets from the red blood cells. The collected platelets and the healing factors within are then injected into the injured area to stimulate healing and tissue regeneration.
While many people believe that they are getting “blood injections,” they are really not. They are getting Platelet Rich Plasma Injections. When the blood is spun it is separated into its various components. Blood is made up of four main components; plasma, red blood cells, white blood cells, and platelets.
There are various ways to prepare PRP, including different kits and manual extraction techniques. The centrifuge is a key device used to separate and concentrate platelets. Techniques such as single-spin or double-spin approaches, as well as filtration methods, impact the quality and potency of PRP. Advances in technology now allow for better platelet capture rates, meaning more platelets can be obtained from the same blood sample compared to older methods, which often required larger draws.
A December 2021 review article (1) in the publication Seminars in musculoskeletal radiology wrote: “Platelets, the namesake component of PRP and an important element of the clotting cascade, also play a significant role in tissue healing, a process that is relatively compromised in ligaments, tendons, and joints, given their relatively poor blood supply.”
Conditions PRP may help with
- Achilles Tendinopathy
- ACL injury and post-reconstruction surgery
- Ankle pain
- Cervical instability
- Elbow pain
- Finger osteoarthritis
- Hamstring injuries
- Hand pain
- Hip osteoarthritis
- Hip labrum tear and post arthroscopic hip pain
- hypermobile Ehlers-Danlos syndrome
- Iliolumbar syndrome
- Iliotibial band syndrome
- Knee osteoarthritis
- Lateral collateral ligament
- Low back pain – Degenerative Disc Disease and herniated disc
- Lumbar stenosis
- Medial collateral ligament
- Meniscus tears
- Neck pain
- Patellar tendinopathy
- Pelvic pain
- Piriformis syndrome
- Posterior cruciate ligament
- Rotator cuff tears and tendonitis
- Sacroiliac joint dysfunction
- Sciatica
- Shoulder dislocation
- Shoulder osteoarthritis
- SLAP tear
- Thumb osteoarthritis
- TMJ
- Toe pain
- Whiplash associated disorders
- Wrist osteoarthritis and pain
PRP growth factors may help ligaments, tendons, and joints heal by bringing healing factors to the damaged area.

In the paper above, emphasis is placed on the tendons and ligaments having a poor blood supply and that is why it is difficult for these soft connective tissues to heal. Ligaments are the rubber band like structures that hold two bones together. Perhaps the most famous ligament is the the ACL or anterior cruciate ligament in the knee. This ligament prevents your shin bone or tibia from sliding out in front of your thigh bone or femur. In many cases of partial tear or where a complete rupture has not occurred, this ligament could heal on its own if it had an adequate blood supply to it. Blood brings healing elements. Unfortunately ligaments do not get a lot of blood to them and they do not heal well on there own. This is why PRP is looked upon as a realistic non-surgical treatment option.
Tendons are in a similar situation. Tendons hold the powerful muscles to the bone. The more famous tendons are the Achilles tendon and the tendons of the rotator cuff. When these tendons are damaged the joint loses its “muscle power.” Muscle power, of course, is an important element in athletes and people who work at physically demanding lines of work.
A 2021 paper (2) describes the benefits of PRP in an athlete population this way:
“Athletes who required a single injection for acute injuries of lower grade returned to sports activity earlier than those who required multiple injections for chronic injuries. We advocate the use of PRP as an adjunct therapy for augmentation of tissue healing for better recovery. PRP injection has optimal effects on sports injuries not responding to conservative management. . .
Comparison to cortisone:
“In certain acute conditions, after a failed conservative management, Corticosteroid injections, known for their anti-inflammatory effect were offered for pain relief. But recently, the use of PRP has been advocated due to its biological healing properties and lesser side effects compared with Corticosteroid injections. The popularity of PRP usage in Orthopaedics has increased owing to the presence of several growth factors released from the alpha granules of platelets.”
“The popularity of PRP usage in Orthopedics has increased owing to the presence of several growth factors released from the alpha granules of platelets.” What does this mean?
The platelets in the blood can also be called “Thrombocytes.” So what do platelets also known as thrombocytes do to fix your damaged joint, neck or back? In an injury event, where something is torn, like skin or ligament or tendon or other soft tissue, the platelets are key players in hemostasis, you would know this as “clotting.” They form “blood clots” to plug up and repair the holes or tears in damaged blood vessels. In this action they also bring in the healing factors to repair the tears.
“Alpha granules” are cellular components of the platelets. This is where the proteins are that drive the platelet healing process. This is what those proteins do:
The platelets contain healing agents, or “growth factors.” Let’s look at some of the growth factors and what they do:
Platelet-derived growth factor
- Platelet-derived growth factor (PDGF) helps direct healing. This is a protein that helps regulate cell growth and division. When there is an injury, more cells are needed for repair and damaged tissue removal. Platelet-derived growth factor is needed by fibroblasts, a specialized cell that helps create collagen, the building block of soft tissues like ligaments and tendons. Research, that I will cite below, has demonstrated that fibroblasts and macrophages (the cells that clear out damaged tissue so new tissue can replace it) can be influenced by the introduction of injection of Platelet-derived growth factor. This influence stimulates chemotaxis (the commands to get cells to the injury), proliferation (the command to create new cells), and gene expression (the command that genes signal to destroy damaged cells, removed the dead damaged cells, bring in the repair cells to rebuild) and bring the beneficial inflammation to accelerate and enhance this healing environment. This is one aspect of how PRP works in chronic injury. The injection of PRP stimulates an acute injury response.
Transforming growth factor beta
- Transforming growth factor beta (or TGF-β) is a polypeptide and is important in tissue regeneration by way of being a communication master. Researchers often talk of the importance of signaling. Signaling is what cells do to tell each other something needs to be done. If these signaling messages stop, are impeded, or disrupted the natural healing cycle does not work. Transforming growth factor beta signaling affects cell differentiation (cells ability to turn themselves into tissue needed for repair), proliferation (ability to make more of themselves), apoptosis (ability to replace dead and damaged cells) and matrix production (make the stuff that the cells need to bind to to stick to damaged areas).
Vascular endothelial growth factor
- Vascular endothelial growth factor (VEGF) is an important protein that helps make new blood vessels. When an area is injured, even in chronic injury, blood vessels are damaged. When the blood vessels are damaged, blood circulation is obviously curtailed. When there is limited circulation – healing factors do not get to the site of the injury, nor does oxygen.
Epidermal growth factor
- Epidermal growth factor plays a key role in tissue repair mechanisms especially influencing fibroblasts (that make collagen) and epithelial cells (that are needed for repair of and creation of new blood vessels.
The research on PRP therapy in orthopedic and regenerative medicine
An October 2023 paper (x) writes: “Level I research supporting the use of PRP in osteoarthritis is available, with a substantial body of evidence supporting its effectiveness in knee and hip osteoarthritis. However, there is limited research on its application in spine, hand, and shoulder osteoarthritis, and no studies supporting its use in elbow and ankle osteoarthritis. High-volume level I research supports its use in lateral epicondylitis, trochanteric bursitis, plantar fasciitis and carpal tunnel neuropathies. Tendinopathies and partial tendon tears have conflicting evidence available, with level I evidence supporting PRP’s use in rotator cuff tendinopathies and tears, with contradictory level I evidence discouraging its use in the patella and Achilles tendinopathies and tears.”
Pretorius J, Habash M, Ghobrial B, Alnajjar R, Ellanti P. Current status and advancements in platelet-rich plasma therapy. Cureus. 2023 Oct;15(10).
PRP for Hip osteoarthritis
Can Platelet-Rich Plasma Therapy be effective in treating hip osteoarthritis and in helping you avoid a hip replacement surgery? The answer in many cases is yes. However, success is dependent on a physical examination and a practice of best diagnosis. The hip is a tricky and complex area filled with many pain generator suspects.
This is a listing of research papers on PRP for hip osteoarthritis over the little more last decade:
Research 2011
- Writing in the Oxford University journal Rheumatology (3) researchers assessed the safety and symptomatic changes in 40 patients receiving platelet-rich plasma (PRP) to osteoarthritis of the hip. In the research, each joint received three hip injections PRP, which were administered once a week.
Results. Statistically significant reductions for pain and improved function were reported at 7 weeks and 6 months.
- Twenty-three (57.5%) patients reported a clinically relevant reduction of pain (45%), Sixteen (40%) of these patients were classified as excellent responders who showed an early pain reduction at 6-7 weeks, which was sustained at 6 months, and a parallel reduction of disability.
Research 2013
- Researchers at the University of Florence found that the majority of patients receiving PRP for hip osteoarthritis had significant pain reduction at 6-7 weeks that was sustained at 6 months, and they also had better range of motion.(4)
Research 2016
- Research from the Rizzoli Orthopedic Institute showed improved findings: “Results indicated that intra-articular PRP injections offer a significant clinical improvement in patients with hip osteoarthritis without relevant side effects.”(5)
Research 2018
- A study (6) from the United Kingdom suggested: “Literature to date concludes that intra-articular platelet-rich plasma injections of the hip, performed under ultrasound guidance to treat hip osteoarthritis, are well tolerated and potentially efficacious in delivering long-term and clinically significant pain reduction and functional improvement in patients with hip osteoarthritis.”
The problems of the hip can often be treated with Platelet-Rich Plasma Therapy. In order to determine if you are a good candidate for this type of procedure, you need to be fully evaluated by a physician who has significant experience with hip pain.
Platelet Rich Plasma Therapy treatments for hip labrum tear
Doctors at the Mayo Clinic examined 8 patients who have previously failed conservative treatments for their hip labrum tear and had later had ultrasound-guided injection of PRP at the site. The patients were assessed for pain and functionality at the start of treatment, then two, six, and eight weeks after injection.
- The findings: Results were good, improvements in pain and function were seen at the two, six, and eight weeks post injection and that “Ultrasound-guided injection of PRP holds promise as an emerging, minimally-invasive technique toward symptom relief, reducing pain, and improving function in patients with hip labral tears.” (23)
Over the years we have seen many patients with hip pain. Many of them having a “hip bursitis,” or more commonly a trochanteric bursitis or iliopsoas bursitis. Sometimes both. The iliopsoas bursitis is felt in the groin area on the inside of the hip. The trochanteric bursitis is felt on the outer part of the hip.
In January 2020, a study published in the medical journal Cureus, (28) offered the following on the comparison of PRP treatments to cortisone:
- 24 patients with greater trochanteric pain syndrome received with PRP treatments or cortisone. The patients in the PRP group had a statistically significant decrease in pain and increase in functionality at the last follow-up (24 weeks post-injection). No complications were reported.
A 2018 study in the Journal of hip preservation (29) made these observations on the use of Platelet Rich Plasma injections for greater trochanteric pain syndrome.
- In most patients improvements were observed during the first 3 months after PRP injection . Significant improvements were reported when patients were followed up to 12 months post treatment. . . Considering these factors, PRP seems a viable alternative treatment with the current evidence in patients with Greater trochanteric pain syndrome not responding to conservative measures.
PRP injections for hip tendinopathy
A July 2021 review paper (34) found good evidence for using platelet-rich plasma in grades 1 and 2 tendinopathy. Shockwave therapy, exercise, and corticosteroids showed good outcomes, but the effect of corticosteroids was short term. A 2018 randomized review study (35) found that patients with chronic gluteal tendinopathy symptoms lasting longer than four months, diagnosed with both clinical and radiological examinations, achieved greater clinical improvement at 12 weeks when treated with a single PRP injection than those treated with a single corticosteroid injection.
PRP for Low Back Pain – Degenerative Disc Disease and Herniated Disc
In 2019 we published our study on the effectiveness of PRP treatments for the patient for chronic low back pain. The study appears in the journal Cogent Medicine.(7)
Our results demonstrated that PRP injections may be a viable conservative approach to treat lower back pain in regards to getting patients back to their everyday activities and improving pain and function.
- Patients quickly returning to everyday activities:
- Our study demonstrated that one, two or three PRP treatments were effective in significantly reducing active pain in the lower back. Additionally, functionality scores were significantly increased showing that patients were able to quickly return to everyday activities.
- An immediate clinical benefit:
- Patients experienced an improvement in resting pain and functionality score after the one treatment, however, statistical significance was demonstrated only after the second and third treatments. Yet, self-reported mean total improvement was 36.33%, 46.17%, and 54.91% at the first, second and third treatments, respectively, suggesting an immediate clinical benefit.
Research has shown (9) PRP to be effective in treating degenerative disc disease (DDD) by addressing the problems of spinal ligament instability and by stimulating the regeneration of the discs indirectly (although discs were not directly injected, they showed an increase in disc height).
The effectiveness of PRP as an alternative to transforaminal steroid injection – Herniated Disc
A May 2021 study (8) doctors tested the effectiveness of PRP as an alternative to transforaminal steroid injection. Transforaminal steroid injection, the doctors noted, is extensively used as a treatment in cases of herniated disc, but is associated with complication and side-effects. In this randomized controlled trial, ultrasound-guided transforaminal injections of either PRP (in 61 patients) or steroid (in 63 patients) were administered to a total of 124 patients who suffer from radicular pain due to lumbar disc herniation. . . No complications were reported. The results showed similar outcome for both transforaminal injections using PRP and steroid in the treatment of lumbar disc herniation, suggesting the possible application of PRP injection as a safer alternative.”
PRP for Low Back Pain – Sacroiliac joint dysfunction
A 2017 study (10) compared the effectiveness of PRP injections versus corticosteroid for sacroiliac joint pain. In this study one group of patients received methylprednisolone, one group of patients received PRP.
- After treatment:
- Intensity of pain was significantly lower in the PRP group at 6 weeks and 3 months as compared to the steroid group.
- The efficacy of steroid injection was reduced to only 25% at 3 months while it was 90% in the PRP group.
- A strong association was observed in patients receiving PRP and showing a reduction of pain of more than 50% from baseline.
- Pain and function scores favored the PRP treatment as well. In the steroid group pain reduction and function improvements were seen up until 4 weeks after treatment and then the effectiveness declined. While the PRP group saw pain and function scores steadily increase at the three month marker.
PRP for Low Back Pain – Iliolumbar syndrome
In a December 2020 study (11), suggested that proper diagnosis of pain sources and PRP injections could significantly help low back pain. In this research low back pain was seen as coming from the iliolumbar ligaments (ligaments that connect the lower spine to the pelvis). The doctors of this study injected PRP in forty-five confirmed patients of iliolumbar syndrome. Out of forty-five patients, forty-two patients showed significant clinico-radiological improvement.
Research has shown Platelet-Rich Plasma Therapy (PRP) to be effective in treating degenerative disc disease by addressing the problems of spinal ligament instability. PRP is an effective means of alleviating back pain because it eliminates pain by healing the underlying issue. As the research above points out, PRP can eliminate the need for surgery.
Platelet Rich Plasma Injections for knee osteoarthritis
Recently, numerous studies have appeared on the effectiveness of PRP in treating knee osteoarthritis.
An editorial in the April 2021 issue of the journal Arthroscopy (12) reflects on the use of PRP injections for knee osteoarthritis:
“Injections for the pain caused by knee osteoarthritis have been the focus of significant research for the last few decades. Systematic reviews and meta-analyses suggest that platelet-rich plasma (PRP) can provide up to 12 months of pain relief in these patients, superior to both cortisone and hyaluronic acid.”
PRP injections significantly improved pain, stiffness and function
A study published in January 2021 (13) issued findings to suggest that PRP injections significantly improved pain, stiffness, function, and disability levels compared with the other injection treatments it was compared against. Intra-articular PRP injection provided better effects than other injections for osteoarthritis patients, especially in knee osteoarthritis patients, in terms of pain reduction and function improvement at short-term follow-up at one month, two months, three months, six months, and 12 months.
In some patients: “The pain symptoms can be alleviated at 3 days after injection”
A January 2022 paper (14) evaluated the effectiveness of platelet-rich plasma injections in people with knee osteoarthritis. All the patients received a PRP injection (3 ml) into the affected knee joint every week for totally three injections. The visual analog scale (VAS) pain 0-10) score and WOMAC (disability) index were used to evaluate knee function before and at three days, one month, and three months after injection. Findings: BEFORE TRETAMENT the (pain) score and (disability) index of patients in the PRP group before treatment were not significantly different from those in the control group. At three days, one month, and three months after PRP treatment, the (pain) score and (disability) index of the PRP group were significantly lower than those of the control group. PRP is effective in treatment of knee osteoarthritis. The pain symptoms can be alleviated at 3 days after injection.”
Effectiveness of PRP injections and compared them to cortisone and hyaluronic acid
A February 2021 (15) study also assed the effectiveness of PRP injections and compared them to cortisone and hyaluronic acid. The researchers noted a specific benefit of treatment: “PRP was proven to halt chondrocytes catabolic activity (breakdown and death of cartilage cells), which is important for the reduction of the chondrocyte apoptosis (death) rate, also resulting in a decrease in the loss of the cartilage matrix secreted by cartilage cells and an increase in cartilage height. (While) the duration of the beneficial effects of PRP injections are unclear, and current evidence indicates that for at least 12 months PRP can improve pain relief and functional improvement in patients with symptomatic knee osteoarthritis, but some (researchers) have described good score values up until 24 months from the beginning of the treatment. Compared to other injective therapies (hyaluronic acid, cortisone, and saline), treatment with PRP was found to be clinically superior in reducing osteoarthritis-related pain symptomatology and increasing the functional outcomes with similar or less risks of adverse events. ”
10 patients who underwent intra-articular PRP injection and 10 patients who received Hyaluronic Acid injection
A September 2021 (16) study compared 10 patients who underwent intra-articular PRP injection and 10 patients who received Hyaluronic Acid injection. At baseline (pre-injection) visit and one, three, six, and 12 months post-injection, clinical assessments were performed using visual analogue scale (VAS) and Knee injury and Osteoarthritis Outcome Score (KOOS) questionnaire.
Results: The PRP treatment was found to be safe and caused no adverse effects. Significant improvements in the majority of KOOS scores and visual analogue pain scale were found throughout the entire 12-month follow-up, following the PRP injections.
Hyaluronic Acid injection, however, caused only one month significant improvement in the majority of patient-reported outcomes. In the majority of visits, the extent of improvements in the scores of Knee injury and Osteoarthritis Outcome Score subscales, as well as the extent of reduction in VAS were significantly greater in PRP recipients, compared to Hyaluronic Acid injection recipients. The ROM in both groups slightly increased after interventions.
Conclusion: Intra-articular injection of PRP or Hyaluronic Acid alleviates symptoms and pain and improves functionality and physical examinations in patients with knee osteoarthritis. However, PRP therapy produces greater and longer-lasting improvements in most of the outcome parameters compared to Hyaluronic Acid.
Effectiveness of PRP in degenerative meniscal tears of the knee
A study from March 2020 (17) examined the effectiveness of PRP in degenerative meniscal tears of the knee. This study included 10 patients with meniscus tear but without knee osteoarthritis. This was a single treatment with follow up at 3 months and 6 months.
- Of the 6 patients who regularly participated in sports were able to recover competition or training.
- In seven patients who underwent MRI follow-up at 6 months, MRI showed stability of the meniscal tears
The doctors were able to conclude of this study: “Intra-meniscal administration of PRP under ultrasound guidance directly into meniscal degenerative lesions is feasible and safe.”
PRP after meniscus surgery
Can PRP accelerate healing after an arthroscopic meniscus repair? It depends on the type of surgery. If the meniscus was repaired with suture and little tissue was removed during the procedure, PRP will most probably be beneficial. If the arthroscopic surgery was a total meniscectomy, then we have to have a realistic expectation of what we are trying to do with the treatment. PRP will not regrow meniscus tissue if there is no meniscus left. PRP can help rebuild the remaining meniscus fragment to an extent. It can help repair it, but it cannot regenerate the “other half,” that was cut out. PRP can be effective in helping stabilize and strengthening the other components of the knee to help accelerate healing after surgery. These would be the ligament and tendon attachments as well as the articular cartilage.
A study from September 2020 (18) looked at the benefits of PRP after a meniscus surgery. Here the suggestion was that while the clinical efficacy of platelet-rich plasma (PRP) as adjuvant therapy in patients undergoing arthroscopic repair of meniscal injury remains controversial. The findings of this meta-analysis suggest that PRP injection can effectively enhance the efficacy of arthroscopic repair of meniscal injury, reduce the failure rate and severity of pain, and improve active flexion.
PRP for patellar tendinopathy
There is limited research as well in the role of PRP in helping patients with patellar tendinopathy. However a 2017 study (36) stated: “These limited studies are encouraging and indicate that PRP injections have the potential to promote the achievement of a satisfactory clinical outcome, even in difficult cases with chronic refractory tendinopathy after previous classical treatments have failed.” One of the studies reviewed was a study from researchers in the Netherlands. In this study, outcomes of patients with patellar tendinopathy treated with platelet-rich plasma injections (PRP) were evaluated to determine whether certain characteristics, such as activity level or previous treatment affected the results. What they found was: “After PRP treatment, patients with patellar tendinopathy showed a statistically significant improvement. In addition, these improvements can also be considered clinically meaningful.”
A 2014 study in The American journal of sports medicine (37) offered these results and assessments:
- “Chronic patellar tendinopathy is one of the most common overuse knee disorders. Platelet-rich plasma (PRP) appears to be a reliable nonoperative therapy for chronic patellar tendinopathy.”
A July 2018 study (38) concluded simply: “Patellar tendons seem to benefit from PRP injections.”
PRP for Elbow Pain

A December 2018 study (19) compared PRP treatments to cortisone for tennis elbow. The results were: “response to PRP seems to be favorable when compared to steroid injection for pain management and for patient-reported outcomes in lateral epicondylitis. PRP injection does not seem to have the potential complications associated with a steroid injection such as skin atrophy, discoloration, and secondary tendon tears.” They also noted that in comparison with extracorporeal shockwave, dry needling, or surgical treatments, (PRP injections in tennis elbow seems to be the best-studied intervention.”
- In the journal The Physician and sports medicine, doctors found steroid could slightly relieve pain and significantly improve function of elbow in the short-term (2 to 4 weeks, 6 to 8 weeks). PRP appears to be more effective in relieving pain and improving function in the intermediate-term (12 weeks) and long-term (half year and one year). Considering the long-term effectiveness of PRP, the researchers recommend PRP as the preferred option for tennis elbow.(20)
Most recently, a June 2021 study (21) also examined the current evidence for the effectiveness of platelet rich plasma (PRP) injections versus corticosteroid injections as treatment interventions for tennis elbow. In this study the researchers concluded corticosteroid injections were more efficacious for short-term pain relief, and PRP injections were more efficacious for long-term pain relief and improved function. PRP injections appear to be a more effective long-term treatment option than corticosteroid injections for those with tennis elbows who did not respond to conservative management.
A 2022 study writes (22): “PRP therapy offers significant pain relief compared to saline control (placebo) when employed in the management lateral epicondylitis. However, we did not note similar improvement in functional outcomes measures. With the available low-quality evidence, PRP is ranked to be the most promising therapy that needs further exploration. Further high-quality (studys) are needed to explore its usefulness in lateral epicondylitis.”
PRP for Shoulder Pain
Rotator Cuff tears and tendonitis
A September 2021 Editorial in the journal Arthroscopy (26) offers this opinion of the effectiveness of PRP injections into the shoulder.
“. . . PRP delivers a high concentration of growth factors, cytokines, and other important inflammatory modulators. Its use is appealing for treating partial-thickness rotator cuff tears, subacromial bursitis, and rotator cuff tendinopathy since rotator cuff tendons often have poor healing capacity due to intrinsic degeneration. PRP has been shown to increase cell proliferation and matrix synthesis in tenocytes, which may aid tendon regeneration and healing.”
A paper (27) evaluating the effectiveness of platelet-rich plasma (PRP) injections in the treatment of common shoulder diseases found: ““PRP injections could provide better pain relief and functional outcomes than other treatments for persons presenting with common shoulder diseases. PRP injections have a greater capacity to improve shoulder-related quality of life than other interventions.” They noted: Compared with placebo and corticosteroid injections, PRP injections provided better pain relief and functional improvement.”
A March 2020 study (33) investigated the effectiveness of platelet-rich plasma (PRP) injection among patients with rotator cuff tendinopathy in comparison with sham injection, no injection, or physiotherapy alone. These researchers found “in the short term (3-6 weeks) and medium term (12 weeks), the effectiveness of PRP injection and control group was indistinguishable in terms of both outcomes (pain reduction and functional improvement). Nevertheless, PRP injection led to significant long-term (more than 24 weeks) pain relief. . . . “PRP injection may provide benefit over the control group (sham injection, no injection, or physiotherapy alone) in reducing pain at long-term follow-up for patients with rotator cuff tendinopathy.”
PRP for Shoulder Dislocation
The shoulder comprises a complex matrix of bone and soft tissue that enables an extreme range of motion. But the price the shoulder pays for that range of motion is a greater risk of chronic injury. The shoulder is held together by soft tissue stabilizers, the ligaments that connect bone to bone. Over the course of time, especially in sports that involve heavy shoulder-to-shoulder contact (such as hockey, lacrosse, football, wrestling, and basketball), the ligaments may stretch out and become “lax.” When the ligaments become lax, the risk of dislocation and separation becomes greater.
In a study published in the British Journal of Sports Medicine, researchers took a look at rugby players with measurable shoulder laxity to gauge the risk of shoulder dislocation. What they found was that 50% of the athletes tested were at significant risk.
It is estimated that 95% of shoulder dislocations occur when athletes suffer a blow to the shoulder that forces the shoulder joint “back” or downward, or occur when they fall to the ground with their arms stretched over their heads.

Ultrasound guided platelet rich plasma injection treatments
An August 2017 (26) study published in the Journal of clinical imaging science found: Ultrasound guided platelet rich plasma injection for partial rotator cuff tears is an effective procedure that leads to significant decrease in pain, improvement in shoulder functions, much cost-effective and less problematic compared to a surgical treatment. “There is conclusive benefit for reducing pain and improving shoulder function in partial rotator cuff tears with ultrasound-guided PRP. . . This study succeeded in demonstrating that those patients receiving PRP injections have decreased pain, healing properties, and superior functional outcomes.”
PRP for Frozen shoulder
Platelet Rich Plasma is seen as a treatment that can help frozen shoulder by addressing the problems of shoulder instability which can cause a thickening of the shoulder capsule.
A January 2021 (30) study suggested PRP injections could help frozen shoulder. In this triple blind study PRP injections were found to be effective in both pain and disability, and showed improvements in a restricted shoulder due to adhesive capsulitis. These findings might point out PRP as a therapeutic option in the management of adhesive capsulitis.
A December 2020 study (31) evaluated the effect of ultrasound guided injection of PRP into the shoulder joint in patients with adhesive capsulitis and compared its effect with that of conventional physiotherapy. Subjects in both groups showed a significant decrease in the pain scores and significant increase in shoulder passive range of motion at all evaluation time points. There was less acetaminophen consumption after PRP injection compared with that after conservative physical therapy.
Platelet Rich Plasma Injections for ankle pain
A February 2021 study (24) tested how effective and safe a single injection of platelet-rich plasma was for patients with ankle osteoarthritis.
- Thirty-nine patients with symptomatic ankle osteoarthritis for at least six months were treated. The patients received a single injection of PRP (3 mL) into the painful ankle(s).
The goal of the study was to see how these patients did at six months after the single injection.
- Results: Significantly improvement in the pain and function scores were noted at 1-, 3-, and 6-month follow-ups.
- Acetaminophen consumption dropped significantly and no serious adverse events occurred.
Achilles tendon injuries
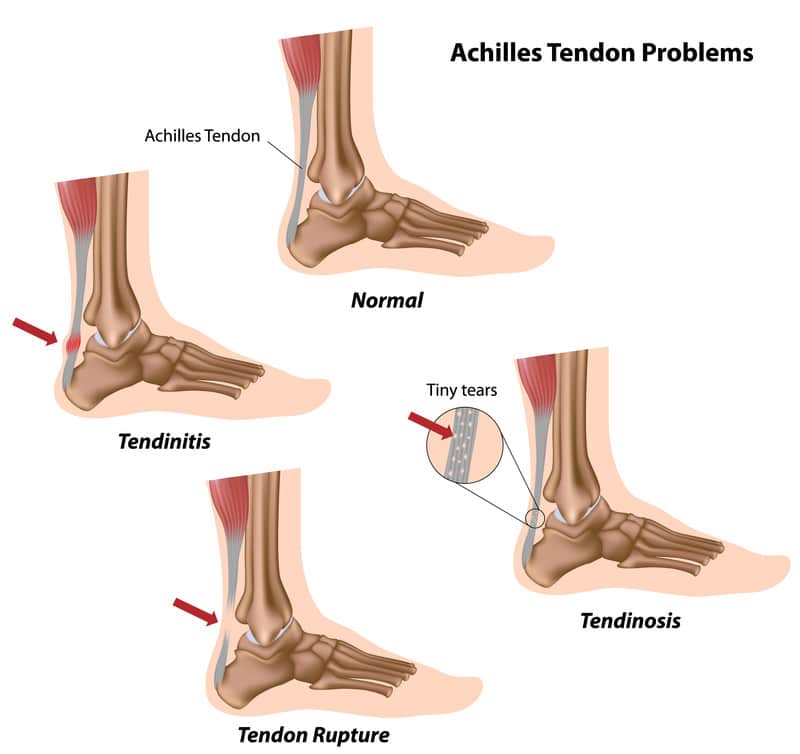
A 2020 study (32) on treating Chronic Achilles Tendinopathy found that PRP showed very promising results demonstrated by a significant improvement in the pain scores. A 2015 study (33) examined 83 Achilles tendons (73 patients, 59 males and 14 females; average age 43) affected by non-insertional CRAT or Chronic Recalcitrant Achilles Tendinopathies. These are difficult to treat cases.
- The patients were treated with a single PRP injection and evaluated with various scoring systems.
- Seventy-six tendons (91.6%) were rated as satisfactory and patients would repeat the treatment.
- Seven tendons (8.4%) were classified as unsatisfactory at the 6 months follow-up and underwent a second PRP injection.
- In addition to this, patients reported no Achilles tendon rupture.
PRP injections for thumb osteoarthritis
A 2021 study (24) compared the effectiveness of PRP injections versus cortisone injections. The summary findings of this study are:
Two groups:
- Group A (16 patients) received 2 ultrasound-guided PRP injections
- Group B (17 patients) received 2 ultrasound-guided intra-articular methylprednisolone and lidocaine injections at a 2-week interval.
- Patients were evaluated prior to and at 3 and 12 months after the second injection.
- After 12 months’ follow-up, the RP treatment has yielded significantly better results in comparison with the corticosteroids, in terms of pain relief, better function, and patients’ satisfaction.
A 2016 study (25) evaluated PRP injections into the trapeziometacarpal (TMC) joint. In this report, ten patients TMC joint osteoarthritis were treated with 2 intra-articular PRP injections four weeks apart. The researchers found improvemnt in pain and suggested “PRP injection for symptomatic trapeziometacarpal osteoarthritis is a reasonable therapeutic option in early stages.”
A 2019 study (42) found that aspiration or arthrocentesis of the jaw joint and platelet-rich plasma injections were effective in reducing pain and joint sound related to TMJD (TMJ Dysfunction) as well as in improving mandibular motion in a maximum follow-up of 24 months.
A 2015 study concluded that patients suffering from TMJ disc dislocation benefited more from PRP injections than from arthrocentesis to manipulate the jaw back in place. Clearly PRP stabilized the joint and reduced chronic instability.(43)
A 2018 study (44) compared PRP injections and hydrocortisone with local anesthetic injections in temporomandibular disorders: Here twenty patients with internal derangements of the TMJ were divided in two groups. In the group of PRP injection, pain was markedly reduced than the group of hydrocortisone with local anesthetic; mouth opening was increased similarly in both groups and TMJ sound was experienced lesser in patients who received PRP.
A June 2019 (45) compared corticosteroids, hyaluronic acid, and platelet-rich plasma for treating TMJ osteoarthritis related pain. Presence of crepitation, loss of function, and loss of strength were assessed before treatment and every month for 3 months. Significant changes were observed in the PRP and hyaluronic acid groups when the patients were evaluated according to the visual analog scale (pain assessment) scores evaluated at different follow-up times for TMJ pain on lateral palpation. However, the findings of this study have shown that intra-articular PRP injections decreased TMJ palpation pain more effectively compared with the hyaluronic acid and corticosteroids groups.
A 2020 study (46) concluded: “Based on current evidence, PRP injections may reduce pain more effectively than placebo injections in TMJ osteoarthritis at 6 months (level of evidence: moderate) and 12 months (level of evidence: moderate) post-injection. This significant difference in pain reduction could also be seen when PRP was compared to hyaluronic acid at 12 months post-injection (level of evidence: low). It can be cautiously interpreted that PRP has a beneficial effect on the relief of TMJ osteoarthritis pain.”
Bone Repair and Regeneration
Investigation into the effectiveness of PRP for bone regeneration have been going on for some time. Here is a sample of the more recent studies as they related to degenerative joint disease.
Research: 2014
“Human bone is a tissue with a fairly remarkable inherent capacity for regeneration; however, this regenerative capacity has its limitations, and defects larger than a critical size lack the ability to spontaneously heal. As such, the development and clinical translation of effective bone regeneration modalities are paramount. One regenerative medicine approach that is beginning to gain momentum in the clinical setting is the use of platelet-rich plasma (PRP). PRP therapy is essentially a method for concentrating platelets and their intrinsic growth factors to stimulate and accelerate a healing response.” (39)
Research 2015
Researchers have confirmed that PRP accelerates the healing and growth of bone in large-bone tumor-created defects and other defects.
“Use of platelet gel as an adjuvant significantly reduces the time required for bone healing following intralesional treatment of benign giant cell tumors, and achieves good functional results without promoting local recurrence.”(40)
Research 2021
“The present systematic review confirmed the continuing interests of PRP as an additional treatment for bone fracture. Preclinical studies highlighted the potential value of PRP as promising therapy for bone fracture. However, the preclinical evidence did not translate into a similar result in the clinical studies. In addition, types of fractures and procedures of PRP preparation are heterogeneous in enrolled studies, which might result in controversial results. Meanwhile, characteristics of PRP, such as platelet concentration, the numbers of leukocytes, still need to be determined and further research is required.” (41)
Do you have questions about PRP? Ask Dr. Darrow
Marc Darrow, MD., JD. has over 23 years experience in regenerative medicine techniques and the treatment of thousands of patients, Dr. Darrow is considered a leading pioneer in the non-surgical treatment of degenerative Musculoskeletal Disorders and sports related injuries. Dr. Darrow has co-authored and continues to co-author leading edge medical research and articles on PRP and other treatment options. Use the form below to ask your qyestion.
References