






Marc Darrow, MD, JD.
The shoulder is a common source of disability resulting from traumatic and degenerate tears of the rotator cuff and biceps tendon, tendinitis, bursitis, subacromial impingement, labral tears, chronic dislocations, and osteoarthritis. Nonoperative management has too often focused on narcotics, other analgesics, anti-inflammatory medications, and steroid injections such as cortisone.
The Leading Causes of Shoulder Pain
- Repetitive overhead sports motions such as pitching, swimming, or the tennis serve.
- Heavy lifting.
- Excessive force or impact on the shoulder such as a fall.
- Degeneration due to aging or overuse.
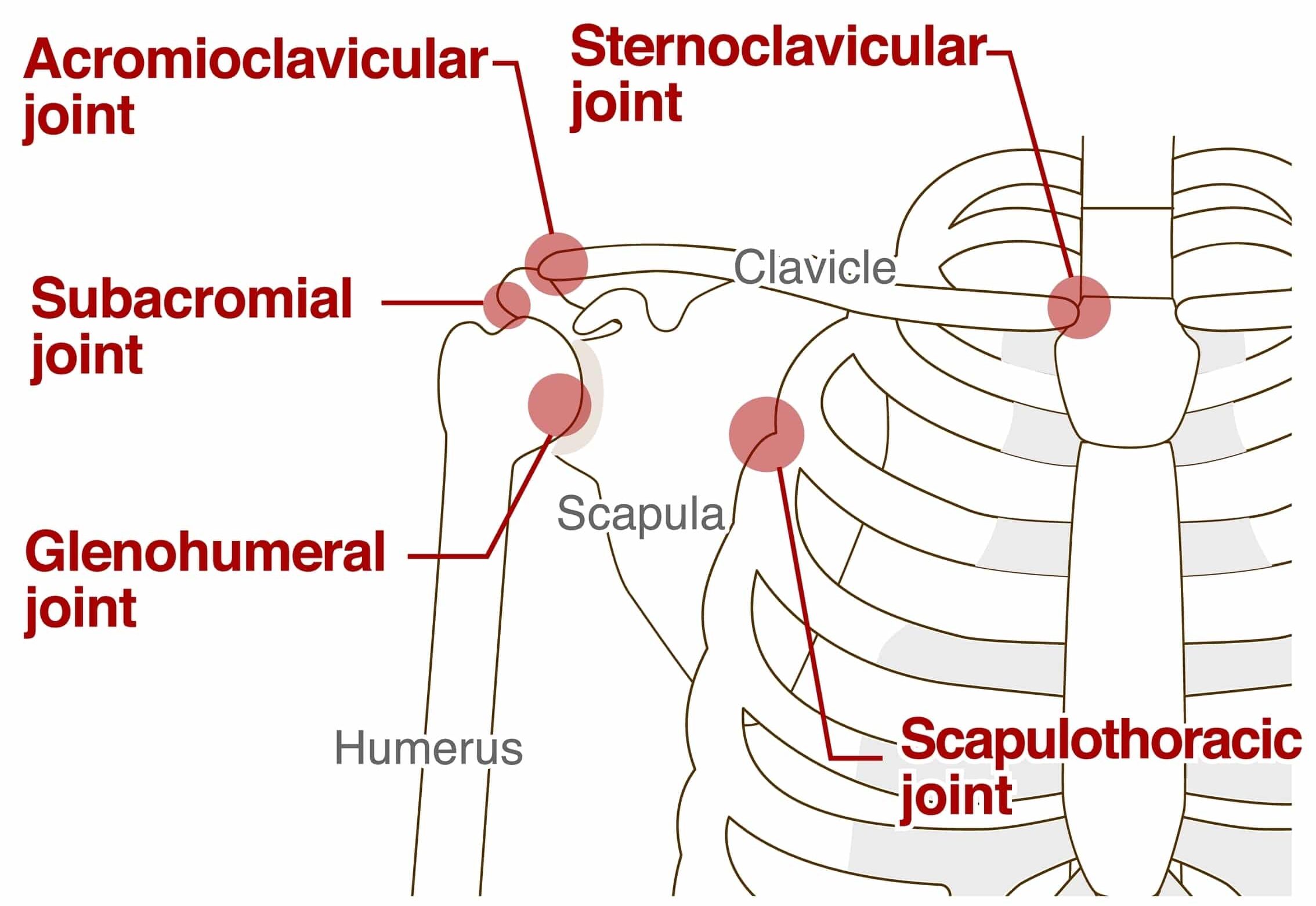
- Narrowing or laxity of the space (acromioclavicular joint) between the collarbone (clavicle) and the top portion (acromion) of the shoulder bone (scapula).
- Abrasion of the rotator cuff surface by the top portion of the shoulder bone (the acromium).
- Non-operative management has focused treatment on painkillers, analgesics, and anti-inflammatory medications. Often—but not recommended by us—corticosteroids are offered in injectable or oral form.
The shoulder is really a combination of the glenohumeral and A/C joints, combined in an intricate arrangement of muscles and tendons that provides the arm a wide range of motion, flexibility and stability. The rotator cuff is a group of four shoulder muscles that surround the top of the upper arm bone, the humerus, and holds it firmly in the shoulder joint. These muscles are responsible for moving the arm in various directions, and unlike the relatively large deltoid muscle of the upper arm, are smaller and generally more vulnerable to injury.
The four muscles and their tendons of the rotator cuff are the supraspinatus, infraspinatus, teres minor and subscapularis. It is the supraspinatus that is most commonly inflamed, worn down, or torn. Keep in mind that tendons connect muscles to bone, and ligaments connect bones to bones. Both tissue types are made of collagen.
Because the supraspinatus and the rest of the shoulder muscles are designed to allow a remarkable array of motion they are frequently subjected to the injuries listed above. Such injuries cause problems of instability or impingement, leading to soft tissue and arthritic pain. The pain may be constant, or may occur only when the shoulder is moved. In any case, shoulder pain that persists more than a few days should be diagnosed and treated as necessary.
The proper diagnosis of shoulder pain is essential in order to determine the root cause of the problem and the proper method of treatment. Because many shoulder conditions are caused by specific activities, a detailed medical history is an invaluable tool. A physical examination should also include screening for physical abnormalities, including swelling, deformity, muscle weakness, and tender areas, along with the range of shoulder motion.
A patient should receive a detailed physical examination. The examination should include screening for physical abnormalities—swelling, deformity, muscle weakness, and tender areas—and observing the range of shoulder motion—how far and in which directions the arm can be moved. In the diagnosis of shoulder pain, a doctor who is assessing non-surgical treatment methods needs to be able to reproduce pain by touching the shoulder and arm. If the doctor can put his/her finger on the exact spot that is causing the pain, then it is likely that the injury involves the soft tissue—muscles, ligaments, and tendons—rather than the bones. These soft tissue injuries are precisely the kinds of injury that respond to regenerative medicine injections.
This article is an overview of the many shoulder problems we see and it is divided into sections.
- Section one is conservative care nonsurgical treatment options for most shoulder pain.
- Section two – failures of arthroscopic and shoulder replacement surgery.
Nonsurgical Conservative care medicine options for shoulder pain and arthritis
Many patients come into our office after a long search for nonsurgical treatments and a long history of conservative care options. Cortisone injections being one of them. In the article below there are many research studies comparing cortisone to other treatments. In this section I will explore other options.
Activity Modification
A top treatment for shoulder pain is also one of the most unpopular treatments. The treatment is called Activity Modification. Activity Modification simply means that you have stopped working or altered the way you work to stop aggravating your shoulder injury, or, you have given up the sport or activity that you love to play in, golf, tennis, rock climbing, surfing, weight training, etc, or you are playing less frequently. Many people do try resting the shoulder. For many people this works very well and they are able to resume playing or working at their physically demanding job. For other however, rest was “only a waste of time.” As soon as these people felt that they have rested their shoulder long enough they tried to resume activities and immediately the shoulder hurt. Is shoulder surgery the only answer for this athlete or laborer who wants a quick return to their sport or work? Many athletes believe that the answer is yes because the common alternative recommendation from their orthopedic specialist of ice, rest, physical therapy, and to wait six months is not the option they want.
Non-steroidal Anti-inflammatory Medications (NSAIDs)
For many people NSAIDS can make their shoulders feel better in the short-term. However, higher doses maybe needed in the long-term to achieve similar results. In a September 2019 study (1) doctors compared ibuprofen and acetaminophen in patients with shoulder pain, specifically pain in the rotator cuff. There were two groups of patients (an ibuprofen group and an acetaminophen group), and there was significant variability in response to these medications. Even if the average pain score was improved, several patients exhibited worsening of their condition.
Physical Therapy
In most cases, before someone can get a recommendation to surgery, they have to complete a course of physical therapy. People who are frequently diagnosed with rotator cuff tendinopathy. I frequently see patients with an MRI of a shoulder tendon tear or an MRI of a problem of chronic tendinopathy. Tendinopathy is a more recent term to describe a chronic pathology of a tendon that causes shoulder pain. The problem of Tendinopathy can be divided into two broad categories:
- Tendinitis means inflammation of the shoulder tendons. This is the characteristic swelling that comes with a worsening wear and tear or acute injury.
- Tendinosis is the “old, nagging injury.” The tendon is injured but the body has given up trying to heal it. It is an injury without inflammation. Why did the body give up? In some of the people we see, it comes as the result of a long and extensive anti-inflammatory or cortisone treatment history.
Many people have had successful physical therapy for treating rotator cuff tendinitis, tendinosis, and shoulder impingement syndrome. The idea of course being the avoidance of movement that causes pain and postural adjustments in the workplace setting to help avoid having the shoulders roll in or sloop. Physical therapy may be less effective or not work at all in situations where the shoulder tendons are stretched or damaged enough that they cannot provide the resistance needed to strengthen the muscles.
Cortisone and Physical therapy
The “go to” injection choice is corticosteroid or more commonly a cortisone shot or non-surgical injection. Many people will not get the cortisone injection alone, it will be coupled with an advanced physical therapy program. The reasoning being that research shows cortisone and physical therapy work better than physical therapy alone. An August 2021 study (2) suggested “(a) combination of corticosteroid injection and physiotherapy is more effective than the physiotherapy alone in resolving the shoulder pain and disability of shoulder.”
Bupivacaine and triamcinolone
An April 2025 study (21) evaluated the effectiveness of fluoroscopy-guided suprascapular (SSN) and subscapular (SCN) articular branch blocks in managing chronic shoulder pain. The primary objective was to assess pain relief using a numerical rating scale (NRS) and functional improvement using Shoulder Pain and Disability Index (SPADI) over 12 weeks.
This study included 70 adults with chronic shoulder pain of more than three months. All patients underwent fluoroscopy-guided suprascapular (SSN) and subscapular (SCN) articular branch blocks with bupivacaine and triamcinolone per site. At 12 weeks, 78 % of patients achieved more than 50 % pain reduction.
Kinesio-taping
An August 2021 paper (3) examined the effectiveness of Kinesio or KT in people suffering from rotator cuff disease. Kinesio Taping (KT) is one of the conservative treatments proposed for rotator cuff disease. As the study authors describe it: “KT is an elastic, adhesive, latex-free taping made from cotton, without active pharmacological agents. Clinicians have adopted it in the rehabilitation treatment of painful conditions, however, there is no firm evidence on its benefits.” Their findings suggest that “Kinesio taping for rotator cuff disease has uncertain effects in terms of self-reported pain, function, pain on motion and active range of motion when compared to sham taping or other conservative treatments as the certainty of evidence was very low. Low-certainty evidence shows that kinesio taping may improve quality of life when compared to conservative treatment. We downgraded the evidence for indirectness due to differences among co-interventions, imprecision due to small number of participants across trials as well as selection bias, performance and detection bias. Evidence on adverse events was scarce and uncertain. Based upon the data in this review, the evidence for the efficacy of KT seems to demonstrate little or no benefit.”
Radiofrequency ablation for chronic shoulder pain
A July 2024 study (19) examined the most recent primary and secondary outcomes of radiofrequency ablation for chronic shoulder pain. Twenty-nine studies were included in the review. Most studies focused on reduction in pain scores, duration of relief, function, and patient satisfaction. In several studies, radiofrequency ablation was compared to conservative options such as physical therapy or corticosteroid injections. Overall, radiofrequency ablation showed positive outcomes in terms of the management of chronic shoulder pain.
Rotator Cuff Tear Treatments – Orthopedic sports medicine

Researchers say that despite increasing medical knowledge, treating shoulder pain—whether in workers, the aging, athletes, or others—remains one of the most challenging tasks in medicine. The problem? Continued shoulder tearing and degeneration after treatment.
Researchers looked at the long-term risks of rotator cuff tear enlargement and symptom progression associated with degenerative asymptomatic tears. (4) They collected patients who had tears but no symptoms in one shoulder, and pain due to rotator cuff disease in the other shoulder. Among the 224 patients in the study, who were followed for an average of five years, there were:
- 118 initial full-thickness tears
- 56 initial partial-thickness tears
- 50 undiagnosed controls
Results:
- Tear enlargement was seen in 49% of the shoulders within an average of 2.8 years.
- Of the 244 subjects, 100 (46%) developed new pain.
Citing this research was a 2022 study (5) which found, “symptomatic rotator cuff tendinopathy progressed to rotator cuff tear based on MRI in 39% of cases at minimum 1-year follow-up, with average follow-up of 3.4 years. This suggests that tendinopathy may be on the spectrum of rotator cuff pathology preceding tear and may progress to a tear if the shoulder remains persistently painful. There were no risk factors found to be associated with progression to tear.” According to a study on athletes, “The results of treatment are not as predictable as the patient, family, trainer, coach, and doctor would like to think.”(6)
Patients at greater risk for rotator cuff revision surgery if they have had a history of cortisone injections
An December 2019 (7) study in the journal Radiology described four main adverse findings that have been structurally observed in patients after cortisone injections.
- Cortisone injections accelerates the progression of degenerative arthritis.
- Cortisone injections cause bone fractures by weakening bone strength.
- Cortisone injections causes bone death and complications of osteonecrosis.
- Cortisone injections cause rapid joint destruction.
In February 2024, (8) researchers building on this research wrote: “Systematic reviews show that the (cortisone) treatment effect is modest compared with intra-articular saline (often considered as placebo) and lasts for 2–4 weeks on average. Potentially as a consequence of limited therapeutic duration, repeated injections are often given up to 4 injections annually. In this context of repeat injections, recent evidence has emerged that intra-articular corticosteroids might be associated with more MRI-assessed quantitative cartilage thickness loss than saline injections.”
Another December 2019 study (9) in the journal Arthroscopy suggests that a steroid injection in the shoulder prior to rotator cuff surgery, puts you at a greater risk for post-surgical shoulder complications and possibly the need for a secondary or revision shoulder surgery. Here is what the study says: “Several recent clinical trials have demonstrated that corticosteroid injections are correlated with increased risk of revision surgery after arthroscopic rotator cuff repair. . . Caution should be taken when deciding to inject a patient (with steroid), and this treatment should be withheld if an arthroscopic rotator cuff repair is to be performed within the following six months.”
A January 2019 study (10) examined the effects of one or multiple corticosteroid injections a patient received for shoulder pain prior to having rotator cuff surgery. The research team found administration of 2 or more injections was associated with a substantially increased risk of subsequent revision rotator cuff surgery.”
However a November 2023 study (11) found that preoperative cortisone injections prior to primary arthroscopic rotator cuff repair did not increase risk of reoperation, infection, or influence patient reported outcomes with a minimum follow-up of 2 years.
Like all injections side effects of cortisone can include infection at the injection site. However, cortisone does have its own history of documented concerns and side-effects.
Bankart Lesion
If you are under 30 years of age, shoulder surgery is typically recommended because younger patients / athletes are much more prone to repeated dislocations than older patients. Until recently it was common in cases of dislocation to immobilize the shoulder for long periods of time. But studies showed that while immobilization helped alleviate the pain of such injuries, it also contributed
to a general weakening of the ligaments and predominance of adhesive capsulitis, or frozen shoulder. Additionally, if a second surgery is needed the patient must be made aware of a high rate of recurrent instability, low rates of return to play, and low clinical outcome scores, or successful treatment. This is why choosing the correct treatment should be given great care.
Bone marrow aspirate concentration (stem cell), Platelet-Rich Plasma Therapy, and Prolotherapy for Rotator Cuff Injury
For many patients, not all, stem cell therapy or bone marrow aspirate concentrate may be effective as non-surgical treatment options. In our research which appears in the peer-reviewed journal Cogent Medicine found here in its entirety: Treatment of shoulder osteoarthritis and rotator cuff tears with bone marrow concentrate and whole bone marrow injections with a June 20, 2019 publication date, we were able to demonstrate:
- Selected patients with rotator cuff tendinopathy and degenerative shoulder disease would benefit from either one and two stem cell treatments. Patients reported significant improvements in resting pain, active pain, and functionality score when compared to baseline.
This is the summary of that research and it explains the bone marrow aspirate concentrate stem cell therapy treatment:
“Human bone marrow offers a promising new therapy for the treatment of chronic shoulder pain. This includes Whole Bone Marrow (WBM) therapy, where the bone marrow is aspirated and reinjected without manipulation, or as Bone Marrow Concentrate (BMC) therapy, where the bone marrow is centrifuged and cleared of red blood cells. Human bone marrow contains many growth factors and important cytokines as well as platelets and mesenchymal stem cells (MSCs). . .
Our study demonstrated that a single injection of Bone Marrow Concentrate or Whole Bone Marrow in the treatment of shoulder osteoarthritis and rotator cuff tears significantly improved resting pain, active pain and functionality score. Patients that received two injections of Bone Marrow Concentrate or Whole Bone Marrow reported greater mean improvement that were also statistically significant when compared to baseline. When injection groups were compared, the two treatment group demonstrated statistically significant improvements in active pain when compared to the one injection group. In addition, there were significant findings across all measure variables when analyzing based on osteoarthritis and rotator cuff tear pathologies. The results of our study show that Bone Marrow Concentrate and Whole Bone Marrow are efficacious in the treatment of rotator cuff tear as well as osteoarthritis with clinically significant benefits to patients after one treatment.”
Similarly, other research has suggested that bone marrow aspirate concentration stem cells showed encouraging results in pain and motion relief for patients with rotator cuff and shoulder
osteoarthritis.(12)
Ultrasound guided platelet rich plasma injection treatments
An August 2017 (13) study published in the Journal of clinical imaging science found: Ultrasound guided platelet rich plasma injection for partial rotator cuff tears is an effective procedure that leads to significant decrease in pain, improvement in shoulder functions, much cost-effective and less problematic compared to a surgical treatment. “There is conclusive benefit for reducing pain and improving shoulder function in partial rotator cuff tears with ultrasound-guided PRP. . . This study succeeded in demonstrating that those patients receiving platelet-rich plasma injections have decreased pain, healing properties, and superior functional outcomes.”
An October 2020 study (14) compared one PRP injection to one corticosteroid injection for pain relief and improved function in patients with rotator cuff tendinopathy and partial thickness rotator cuff tears. After the one injection, patients were followed and results recorded at six weeks, three and twelve months post-injection. The researchers observed that patients with partial rotator cuff tears or tendinopathy experienced improvement in pain after both ultrasound-guided corticosteroid and PRP injections. However the patients who received PRP had superior improvement in pain and function at short-term follow up (3 months). One injection of PRP is not the way we offer the treatment.
The video below demonstrates the treatment
Shoulder Tendinitis / Tendinosis / Bursitis – platelet-rich plasma injections
Tendinitis in the shoulder occurs from inflammation of the tendons as a result of the wearing process that takes place over a period of time, or from an unusual load on the joint, or awkward movement, or fall. Although doctors and patients tend to identify any pain originating from the tendons as tendinitis, research recently has found that tendinitis is the microtearing of the tendon with inflammation. On the other hand, tendinosis is the wearing of the tendon’s collagen without inflammation and usually occurs after the inflammatory process ends. Either way, healing can occur with regeneration of the tendon’s collagen.
Sometimes excessive use or injury of the shoulder leads to inflammation and swelling of the subdeltoid bursa, a condition known as bursitis. Bursae are fluid filled sacs located around the body and joints. They cushion tendons, ligaments, and muscles from bones. Bursitis often occurs when the sac is inflamed and may be in association with rotator cuff tendinitis. Symptoms of shoulder bursitis include mild to severe pain, limiting the use and range of motion of the shoulder. In extreme cases the joint capsule stiffens and range of motion is lost. This condition is known as “frozen shoulder,” also referred to by doctors as adhesive capsulitis which I discuss below.
In a July 2021 study (15), study researchers wrote: “Rotator cuff tendinitis has been treated using various methods including physiotherapy, steroid injections and recently platelet rich plasma (PRP). Most of these methods aim at giving symptomatic relief rather than addressing the pathology (the cause of the problem). There is no clear consensus over the benefit of using PRP for tendinitis. (The authors) decided to do a prospective clinical study to demonstrate the efficacy of PRP and study the functional outcome in the treatment of rotator cuff tendinopathy.
- Patients with shoulder pain for more than three months not responding to NSAIDs or physiotherapy with a diagnosis of rotator cuff tendinitis, confirmed by MRI, were included in the study.
- Thirty patients received an ultrasound guided PRP injection in the subacromial space followed by a six-week exercise program.
- Patients were followed-up at three, six and 12 weeks and were assessed clinically using the Pain and functional scoring systems.
The ten point Visual Analogue System score 0 being no pain and 10 being unbearable pain improved from a pre injection score of 7.4 (significant pain) to a score of 1.9 (little pain) in the 12th week. The mean SPADI (Shoulder Pain and Disability Index) score and Constant (pain and shoulder rotation score the lower the number the better) score improved significantly.
Conclusion: “Platelet Rich Plasma injections showed good to excellent early results, in patients with rotator cuff tendinopathy with improvement in VAS, SPADI and Constant scores.”
Orthopedic sports medicine – SLAP Lesions (Superior Labral Anterior Posterior) platelet-rich plasma injections

The surgical treatment of labral (tissue around shoulder joint) SLAP tears continues to be challenging for both physicians and patients. Of course, it becomes much more challenging to the patient if the surgery does not work to the patient’s expectations. A 2016 paper stated that tears of the superior labrum involving the biceps anchor are a common occurrence, especially in athletes, and may highly impair shoulder function. If conservative treatment fails, successful arthroscopic repair of symptomatic SLAP lesions has been described in the literature, particularly for young athletes.
However, the results for athletes whose sport involves throwing are less successful, with a significant proportion of patients who will not regain their pre-injury level of performance. The clinical results of SLAP repairs in middle-aged and older patients are mixed, with worse results and higher revision rates compared to younger patients. In this population, tenotomy (surgical division of a tendon) or tenodesis (suturing of the end of the biceps tendon to the bone) are viable alternatives to SLAP repairs in order to improve clinical outcomes.(16) In tenodesis, the surgeon moves the
bicep tendon attachment to a different place on the bone (usually as part of a more complex surgery).
SLAP (Labral) Lesions May Actually be Rare Injuries
Too many times I see patients complaining of continued pain after a failed labral repair. Was the “torn” labrum the pain generator? Probably not, or perhaps the surgery may have caused more damage. Consider what happens when a knife cuts into the body and tools are used to “repair” the area. And why is it that I often see patients with pain and loss of range of motion that show no pathology on MRI. I am pressing you to understand that as doctors we really don’t always know exactly what is going on, even after the history, physical, and diagnostic films. That’s why my first law of medicine is to be conservative, and do no harm. And with this in mind in light of too many surgeries being done, why not regenerate the tissue instead of cutting it out?
Is shoulder surgery the answer for the athlete who wants a quick return to their sport? For many athletes and non-athletes, the answer is yes, because the alternative recommendations from their orthopedic specialist of ice, rest, physical therapy and waiting six months is not the option they want. And honestly, even today, most surgeons—even those who do PRP and Stem Cells—do not believe alternative therapies work, using them simply as a way to bring patients into the office. When the pain persists after an incomplete course of treatment, surgery is then recommended.
Unfortunately, the process of tissue regrowth often takes several treatments over several weeks. I always suggest nonsurgical options, since, as noted at the start of this book, I personally had a failed shoulder surgery that made my shoulder much worse. After surgery, my arm filled with fluid, I had a fever, and large blisters developed on my arm and shoulder. I liked my surgeon, who was my professor while I was doing orthopedic surgery in my training—but at that point I realized that surgery was a mistake in many instances, and I questioned whether I still wanted to make it my lifetime work. When I learned about regenerative medicine, I injected my own shoulder and the pain was gone when I awakened the next morning. My shoulder remained pain-free for twelve years until I reinjured it, at which point I repeated the injections, and again healed my own shoulder. It has been pain free since then.
It takes nine months to recover from SLAP surgery to return to sport – unless you are a throwing athlete or pitcher
A December 2019 paper (17) offered these timetables for a return to sport in evaluating individuals undergoing arthroscopic SLAP repair shoulder orthopedic surgery. This research encompasses 22 previously published articles involving a total of 944 patients undergoing arthroscopic SLAP repair.
- Of the total included patients, 270 were identified as overhead athletes, with 146 pitchers.
- Across all patients, 69.6% (657/944 patients) of individuals undergoing arthroscopic SLAP repair returned to sport.
- There was a 69.0% (562/815 patients) return to previous level of play, with a mean time to return to sport of about nine months.
- The return-to-sport rate for pitchers compared with the return-to-activity rate for nonpitchers, encompassing return to work and return to sport, was 57.5% (84/146 patients) and 87.1% (572/657 patients), respectively, after arthroscopic SLAP repair.
Conclusion: “Arthroscopic SLAP repair is associated with a fair return to sport, with 69.6% of individuals undergoing arthroscopic SLAP repair returning to sport. SLAP repair in pitchers has significantly decreased return to sport in comparison with nonpitching athletes. Athletes on average return to sport within 9 months postoperatively.”
Shoulder Impingement: Surgery Not Often the Answer
Shoulder impingement surgery may not be the fastest way back to health. A patient with problems of the rotator cuff or shoulder impingement may think that surgery will be a quick fix. However,
surgery is an invasive procedure that often requires lengthy recovery and physical therapy even if it is successful. Further, even “successful” surgery may not relieve the pain, and shoulder weakness can remain.
Although “impingement” refers specifically to pressure on the tendons and bursa in the shoulder, it is a generalized term often used to refer to shoulder pain of unknown origin. Other terms used are tendinitis, tendinosis, and bursitis, when none of these are actually proven as pain generators.
Shoulder Dislocation
The shoulder comprises a complex matrix of bone and soft tissue that enables an extreme range of motion. But the price the shoulder pays for that range of motion is a greater risk of chronic injury. The shoulder is held together by soft tissue stabilizers, the ligaments that connect bone to bone. Over the course of time, especially in sports that involve heavy shoulder-to-shoulder contact (such as hockey, lacrosse, football, wrestling, and basketball), the ligaments may stretch out and become “lax.” When the ligaments become lax, the risk of dislocation and separation becomes greater.
In a study published in the British Journal of Sports Medicine, (20) researchers took a look at rugby players with measurable shoulder laxity to gauge the risk of shoulder dislocation. What they found was that 50% of the athletes tested were at significant risk.
It is estimated that 95% of shoulder dislocations occur when athletes suffer a blow to the shoulder that forces the shoulder joint “back” or downward, or occur when they fall to the ground with their arms stretched over their heads.
Chronic Shoulder Dislocation Treatment, Platelet-rich plasma treatment
Traumatic shoulder dislocation is a frequent injury in the sports population. An acute shoulder dislocation often means a one-time traumatic episode, whereas chronic shoulder instability indicates multiple recurrent dislocations.
Following an initial shoulder dislocation, doctors debate whether or not to perform surgery to prevent recurrence. If there is an accompanying labral or tendon tear, that can be addressed along with tightening of the capsule around the joint. This can lead to a loss of range of motion. I have used Stem Cell Therapy with platelets (both are in the bone marrow) or just PRP from the blood, both with good results, to tighten the shoulder after a failed surgery for chronic dislocations.
If the patient is under 30 years of age, shoulder surgery is typically recommended by surgeons because younger athletes are much more prone to repeated dislocations than older athletes.
Until recently, it was common in cases of dislocation to immobilize the shoulder for long periods of time. But studies showed that while immobilization helped alleviate the pain of such injuries, it also contributed to a general weakening of the ligaments and predominance of “adhesive capsulitis,” where the arm is frozen (frozen shoulder) and can no longer be lifted.
Surgery for shoulder dislocation can be effective for some but, as always, surgery should be considered a last option because of issues of complications, downtime (immobilization), and—for both the “weekend warrior” and the professional athlete—a weakening of the shoulder through the removal of or damage to other connective tissue in the surgical process.
The key to avoiding shoulder surgery or shoulder separation requiring surgery is to strengthen the shoulder girdle. This can be accomplished by working the strong shoulder muscle group and by
treating the weakened shoulder ligaments with injections of regenerative medicine.
To understand the importance of having strong ligaments to hold the shoulder together, the patient needs to understand that the severity of the shoulder dislocation is measured by the degree of injury to the ligaments and the amount of instability of the joint.
Shoulder Separation
The acromioclavicular (AC) and the coracoclavicular (CC) ligaments hold the shoulder together at the point where the collarbone (clavicle) and the top (acromion) of the shoulder meet. This joint can also be traumatically separated. I see this most commonly in bicycling accidents in which the patient has flown over the handlebars and landed on the shoulder.
This is a very small joint that heals well with regenerative medicine.
- In type I level separation, the AC is partially torn; the CC is not.
- In type II separation, the AC is completely torn; the CC is partially or not torn.
- In type III separation, both ligaments are completely torn.
With this injury one can often see the collarbone sticking up above the top of the shoulder. Obviously, the more significant the tearing, the longer the athlete is out of their sport. Untreated shoulder instability can lead to an alteration of an athlete’s game to protect the sore shoulder, or, worse, chronic shoulder separation that can keep athletes away from their sport for significant
amounts of time. Bone Marrow Stem Cell Therapy and PRP use the patient’s own cells to repair and rebuild ligaments and the joint itself.
Research on Platelet Rich Plasma injections – PRP may help frozen shoulders
Information on Frozen shoulder – Adhesive capsulitis and Platelet Rich Plasma Therapy
There are many treatments that can work for to get the shoulder “unstuck” or “unfrozen” as described in the above research. Platelet Rich Plasma is seen as a treatment that can help frozen shoulder by addressing the problems of shoulder instability which can cause a thickening of the shoulder capsule. A January 2021 (25) study suggested PRP injections could help frozen shoulder.
This was triple blind study, the doctors did not know what they were injecting, the patients didn’t know what they were being inject with and the researcher analysis did not know what treatment offered the results they were examining. The researchers found PRP injections were found to be effective in both pain and disability, and showed improvements in a restricted shoulder due to adhesive capsulitis. These findings might point out PRP as a therapeutic option in the management of adhesive capsulitis.
Summary
A patient with problems of the rotator cuff or shoulder impingement may believe surgery is still the best answer for them, and maybe it is. However, surgery is a still an invasive procedure that requires lengthy recovery and physical therapy even if successful. Further, even successful surgery has been shown to not always relieve all preexisting pain and shoulder weakness can remain. Complications may also include nerve damage.
Shoulder injuries can be divided into two groups —the more common and the first to be discussed is the wear and tear injury to the tendons. The shoulder tendons are main players in rotator cuff problems, shoulder impingement, osteoarthritis, and disorders of pain and weakness that get worse over time.
The symptoms of tendon weakness and injury are many and include inflammation of the tendons (tendinitis), and/or bursitis– inflammation of the bursa, the protective sac that sits between the bones of the shoulders and allows the tendons the space they need to move.
All medical professionals would agree that treating the tendons and allowing the tendons to function normally would be the optimal treatment in shoulder pain, but that is where the agreement ends. Surgeons will insist that surgery after failed conservative treatments is the way to go while other doctors have pioneered quicker and less intrusive methods.
Bone Marrow stem cell therapy and Platelet Rich Plasma Therapy are injection techniques that can accelerate the body’s own inflammatory response to repair the tendons. In the case of Stem Cell Injection Therapy, the stem cells can morph into, and rejuvenate the tissue that is damaged.
By isolating the areas of the tendons that are damaged and injecting these spots, the doctor is focusing the natural injury repair mechanism of the body to the spot of deterioration. The treatment is the new, controlled inflammation and tissue regrowth. This will stimulate a new collagen matrix, making the tendons stronger, thicker, and restoring them to their normal pain-free state. To any athlete stronger is always the best option.
Side-effects are also limited and are typical of any injection side effect including infection or swelling or discomfort at the injection site. and in many cases the athlete can continue their activities during treatments.
Call for a free phone consultation with our staff 800-300-9300
References
1 AlRuthia Y, Alghadeer S, Balkhi B, Almalag HM, Alsobayel H, Alodaibi F, Alayoubi F, Alkhamali AS, Alshuwairikh S, Alqahtani FN, Alsanawi H. Efficacy of acetaminophen versus ibuprofen for the management of rotator cuff-related shoulder pain: Randomized open-label study. Saudi Pharmaceutical Journal. 2019 Sep 1;27(6):882-8.
2 Khan RD, Shahzad K, Khan S, Israr M, Zahid FM. Comparison of physiotherapy with and without intra-articular corticosteroid injection for treatment of frozen shoulder: A comparative study. JPMA. The Journal of the Pakistan Medical Association. 2021 Aug;71(8):S17-21.
3 Gianola S, Iannicelli V, Fascio E, Andreano A, Li LC, Valsecchi MG, Moja L, Castellini G. Kinesio taping for rotator cuff disease. The Cochrane Database of Systematic Reviews. 2021 Aug 8;8:CD012720-.
4 Keener JD, Galatz LM, Teefey SA, Middleton WD, Steger-May K, Stobbs-Cucchi G, Patton R, Yamaguchi K. A prospective evaluation of survivorship of asymptomatic degenerative rotator cuff tears. The Journal of bone and joint surgery. American volume. 2015 Jan 21;97(2):89.
5 Quinlan NJ, Frandsen JJ, Smith KM, Lu CC, Chalmers PN, Tashjian RZ. Conservatively treated symptomatic rotator cuff tendinopathy may progress to a tear. Arthroscopy, sports medicine, and rehabilitation. 2022 Aug 1;4(4):e1449-55.
6. Garbis NG, McFarland EG. Understanding and evaluating shoulder pain in the throwing athlete. Phys Med and Rehabil Clinics of North Am. 2014; 25 (4): 735. doi:10.1016/j.pmr.2014.06.009.
7 Kompel AJ, Roemer FW, Murakami AM, Diaz LE, Crema MD, Guermazi A. Intra-articular corticosteroid injections in the hip and knee: perhaps not as safe as we thought?. Radiology. 2019 Dec;293(3):656-63.
8 Guermazi A, Hunter DJ, Kloppenburg M. Debate: Intra-articular steroid injections for osteoarthritis–harmful or helpful?. Osteoarthritis imaging. 2023 Sep 1;3(3):100163.
9 Puzzitiello RN, Patel BH, Nwachukwu BU, Allen AA, Forsythe B, Salzler MJ. Adverse impact of corticosteroid injection on rotator cuff tendon health and repair: A systematic review. Arthroscopy: The Journal of Arthroscopic & Related Surgery. 2019 Dec 17. platelet-rich plasma treatment
10 Desai VS, Camp CL, Boddapati V, Dines JS, Brockmeier SF, Werner BC. Increasing numbers of shoulder corticosteroid injections within a year preoperatively may be associated with a higher rate of subsequent revision rotator cuff surgery. Arthroscopy: The Journal of Arthroscopic & Related Surgery. 2019 Jan 1;35(1):45-50.
11 Smith JT, Pill SG, Eggert KA, Brignull CG, Adams KJ, Wyland DJ, Tolan SJ, Thigpen CA, Kissenberth MJ. Corticosteroid injection prior to surgery had no effect on 2-year outcomes following arthroscopic rotator cuff repair. JSES international. 2024 Jan 1;8(1):75-9.
12 Mora MV, Ibán MA, Heredia JD, Laakso RB, Cuéllar R, Arranz MG. Stem cell therapy in the management of shoulder rotator cuff disorders. World Journal of Stem Cells. 2015 May 5;7(4):691.
13 Sengodan VC, Kurian S, Ramasamy R. Treatment of Partial Rotator Cuff Tear with Ultrasound-guided Platelet-rich Plasma. J Clin Imaging Sci. 2017 Aug 14;7:32.
14 Kwong CA, Woodmass JM, Gusnowski EM, Bois AJ, Leblanc J, More KD, Lo IKY. Platelet Rich Plasma in Patients with Partial Thickness Rotator Cuff Tears or Tendinopathy Leads to Significantly Improved Short-Term Pain Relief and Function Compared to Corticosteroid Injection: A Double-blind Randomized Controlled Trial. Arthroscopy. 2020 Oct 27:S0749-8063(20)30893-8. doi: 10.1016/j.arthro.2020.10.037.
15 Pritem AR, Abraham VT, Krishnagopal R. Early Clinical and Functional Outcome of Rotator Cuff Tendinopathy of the Shoulder Treated with Platelet Rich Plasma Injection. Malaysian Orthopaedic Journal. 2021 Jul;15(2):55.
16. Brockmeyer M, Tompkins M, Kohn DM, Lorbach O. SLAP lesions: a treatment algorithm. Knee Surg Sports Traumatol Arthrosc. 2016 Feb;24(2):447-55.
17 Thayaparan A, Yu J, Horner NS, Leroux T, Alolabi B, Khan M. Return to sport after arthroscopic superior labral anterior-posterior repair: A systematic review. Sports health. 2019 Nov;11(6):520-7.
18 Ünlü B, Çalış FA, Karapolat H, Üzdü A, Tanıgör G, Kirazlı Y. Efficacy of platelet-rich plasma injections in patients with adhesive capsulitis of the shoulder. International Orthopaedics. 2020 Nov 18:1-0.
19 Jain E, O’Connor IT, Tram JK, Varlotta CA, Fiala KJ, Asaad FS, Chitneni A, Abd-Elsayed A. Radiofrequency ablation for shoulder pain: an updated systematic review. Annals of Palliative Medicine. 2024 Jul 31;13(4):96375-975.
20 Cheng SC, Sivardeen ZK, Wallace WA, Buchanan D, Hulse D, Fairbairn KJ, Kemp SP, Brooks JH. Shoulder instability in professional rugby players—the significance of shoulder laxity. Clinical Journal of Sport Medicine. 2012 Sep 1;22(5):397-402.
21 Jain A, Jithin KJ, Kumar H, Sarawagi R, Kaushal A, Barasker SK. Fluoroscopy-guided suprascapular and subscapular articular nerve blocks for chronic shoulder pain: A 12-week observational study. Interventional Pain Medicine. 2025 Jun 1;4(2):100582.