






Marc Darrow, MD.
There are many types of arthritis, but most often in the shoulder, arthritis or osteoarthritis is triggered by an initial trauma or degenerative “wear and tear” of the tissues of the joint, causing inflammation, swelling and pain. Often people will react by instinctively limiting their shoulder movements in order to lessen the pain. This can lead to a tightening or stiffening of the soft tissue parts of the joint, resulting in yet further pain and restriction of motion. In the worst cases, frozen shoulder or adhesive capsulitis occurs and the arm can not be moved.
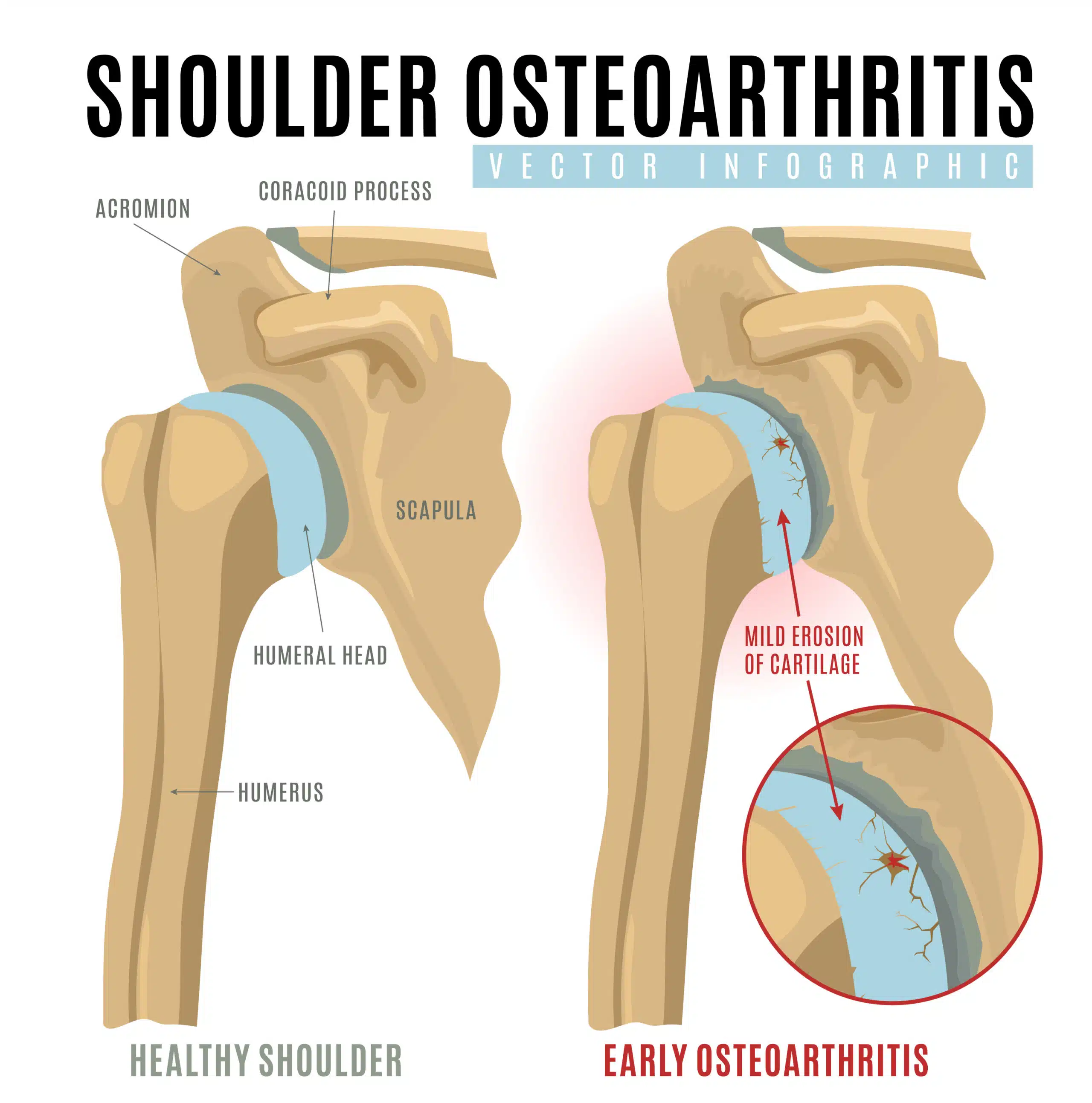
Glenohumeral osteoarthritis is the degenerative breakdown of the ball and socket of the shoulder. If you went to the doctor with shoulder pain, and you had a shoulder MRI, and that MRI revealed shoulder osteoarthritis, the next discussion you will probably have with your doctor is what can you do about it? That answer is not clear cut. What treatments you take can be influenced by the amount of pain and function that you have.
The shoulder examination
A physical examination should include screening for physical abnormalities—swelling, deformity, muscle weakness, and tender areas—and observing the range of shoulder motion—how far and in which directions the arm can be moved. Although x-rays may be helpful in defining problems, more elusive ones may require computerized tomography (CT scan), which provides a more detailed view of the bones. Electrodiagnostic studies such as the electromyogram (EMG) and a nerve conduction study can indicate whether pain or weakness in the area is coming from a pinched nerve in the neck, or a peripheral nerve injury away from the neck, or down the arm. Magnetic Resonance Imaging (MRI) and ultrasound are other safe and effective diagnostic tools, providing images of the soft tissues without using radiation. An arthrogram is an x ray, CT or MRI in which dye is injected into the joint for added contrast. However, as outlined in other sections of this website, studies have shown that the advanced technologies commonly used to diagnosis injuries are grievously insufficient to show where the pain is coming from.
Treatment recommendations in the medical research
Doctors at the Mayo Clinic, published July 2022 recommendations (1) for the treatment of shoulder osteoarthritis. They write: “Glenohumeral osteoarthritis has proven to be a major contributor to shoulder joint pain and dysfunction in the elderly. There are several conditions about the shoulder that contribute to the development of glenohumeral osteoarthritis, which includes traumatic injuries, rotator cuff pathology, glenohumeral instability, glenoid dysplasia, and osteonecrosis. When glenohumeral osteoarthritis pain is refractory (not responding) to conservative treatment, intra-articular injections and surgery can be performed. The radiologist should be aware of the varying types of shoulder arthroplasties, what preoperative findings influence that decision and the expected postoperative appearance of the differing components.”
A February 2022 paper (2) examined the treatment options for older patients with shoulder or glenohumeral osteoarthritis and provides the basis of treatment. Many of the people who come to us for care options have already followed and unfortunately failed many of these interventions.
Here are the learning points of this research:
Glenohumeral osteoarthritis (arthritis of the ball and socket of the shoulder) is a common cause of shoulder pain and is characterized by articular cartilage thinning, glenoid bone loss and deformity, osteophytosis (bone spurs), and other associated changes.
Non-pharmacological treatment options may serve as adjuvants to other therapies and should be incorporated for a more holistic approach to management. Pharmacological treatments include oral agents such as acetaminophen, non-steroidal anti-inflammatory drugs (NSAIDs), opioids, corticosteroids and antidepressants.
Intra-articular injections such as platelet-rich plasma, cortisone, and hyaluronic acid are usually used to control symptoms in moderate to advanced arthritis or in non-surgical candidates. Other non-surgical treatment options include suprascapular nerve block and radiofrequency ablation, and these options have been studied on different levels of evidence. Surgical treatment of Glenohumeral osteoarthritis is reserved for patients who do not respond to conservative management or who suffer from debilitating symptoms that severely impair their quality of life.
We also see people who already had many surgeries and now so little is left of their shoulder they have to have a shoulder replacement. I myself had arthroscopic shoulder surgery many years ago. It did not help me and it took a year of rehab just to get it back to what it felt like just before the surgery. I see this in people all the time. They have a shoulder surgery, they rehab for a year, the shoulder still hurts, they have another shoulder surgery, they rehab for one year then it is deiced that they have reached the point of no return, shoulder replacement, they only decision left is reverse shoulder replacement or a shoulder replacement. So now that this person is waiting to get a shoulder replacement, what happens next? For some, cortisone injections to hold them over. Cortisone injections, as it has been demonstrated, can accelerate avascular necrosis or bone death. So a person has had two surgeries and they may have no cartilage left, now they are getting cortisone, now they will have no bone left.
Conservative treatment is this a realistic plan to get pain-free range of motion?
Physical therapy for shoulder arthritis
Here is a summary from a June 2023 paper from a team of international doctors (3) to include a description and goals of physical therapy:
- “Physical therapy is performed to (1) decrease pain, (2) increase shoulder range of motion, and (3) protect the glenohumeral joint. Physical therapy may be effective for motion pain rather than rest pain.”
- To increase shoulder shoulder range of motion, the soft tissues (ligaments, tendons, labrum) responsible for the range of motion loss need to be identified and targeted for intervention.
- To protect the glenohumeral joint, rotator cuff strengthening exercises are recommended.
The use of anti-inflammatories is recommended to reduce pain and lessen the inflammation in the shoulder. This “interrupts the chronic inflammatory state in the joint and in turn enables pain-free physical therapy.”
Does prior cortisone injections increase risk of shoulder replacement complications?
This is a widely debated controversy in medicine with research demonstrating increased post-surgical complication when the patient had prior cortisone injections and other research suggesting post-surgical complication risk is minimal.
A June 2024 study (4) suggests, when cortisone is used, judiciously, prior to shoulder replacement, post surgical complications are minimal. Here are this study’s highlights.
The authors write: “Recent studies in the shoulder arthroplasty (replacement) literature as well as applied from the hip and knee literature have focused on the risk of periprosthetic infection. Literature is lacking as to whether the judicious use of corticosteroids in the year prior to arthroplasty influences patient-reported outcomes (PROs). The purpose of this study was to determine if preoperative CSIs prior to shoulder arthroplasty affected 2-year patient reported outcomes.”
The data:
- Researchers examined the patient records of 230 patients who had shoulder replacement or reverse total shoulder replacement.
- Of the 230 patients – 134 patients had cortisone injections prior to surgery and 96 did not.
- In assessing outcomes, the researchers found the 134 patients who received an injection within 12 months prior to anatomic and reverse total shoulder replacement, do not report worse pain and function outcomes during a minimum of 2-year follow-up than the 96 patients who did not have a cortisone injection. Although more complications occurred in the injection group, it did not reach statistical significance and warrants further study in a larger population.
Intra-articular hyaluronic acid injections in the shoulder
A June 2023 review study in the Journal of orthopaedic research (5) researchers evaluated the current evidence regarding the effectiveness of intra-articular hyaluronic acid on pain relief in patients suffering from glenohumeral osteoarthritis and found that intra-articular hyaluronic acid injections might be effective on pain relief with significant improvements compared to baseline and compared to corticosteroid injections in patients affected by glenohumeral osteoarthritis.
A November 2022 paper (6) tested the effectiveness of ultrasound-guided glenohumeral joint injections of Leukocyte-Poor Platelet-Rich Plasma against Hyaluronic Acid in the ttreatment of Glenohumeral Osteoarthritis. This was a randomized, double-blind controlled trial.
- Seventy patients with chronic glenohumeral osteoarthritis were randomly assigned to receive a single injection of Hyaluronic Acid or Leukocyte-Poor Platelet-Rich Plasma.
- Main outcome measures: Shoulder Pain and Disability Index (SPADI), American Shoulder and Elbow Surgeons (ASES) score, current/average numerical rating scale (NRS) pain scores, satisfaction, and side effects were assessed at the 5 follow-up time points over 12 months.
- There were no significant between-group differences regarding SPADI, ASES, and current/average NRS pain scores at any time point up to 12 months post-injection. However, significant improvements in SPADI, ASES, and current/average NRS pain scores were observed in both groups starting at 1 or 2 months. These improvements were observed regardless of osteoarthritis severity. For patients who received LP-PRP, there was no effect of platelet yield on outcomes. Side effect and satisfaction rates were similar between groups.
Can people who had previous failed glenohumeral arthroscopic shoulder surgery have a successful shoulder replacement?
Many people come into our office with a history of failed shoulder surgeries. Some will be in our office because they are exploring options to the “final” surgical recommendation, a total shoulder replacement. For some, with the history of failed surgery, they have obvious concerns. Being a failed should surgery patient myself, I would have concerns too about another surgery.
A June 2021 paper (7) examined if people who had a failed arthroscopic shoulder surgery would be at risk for a failed total shoulder replacement. In this study of 56 patients all under the age of 70, doctors examined 19 patients had the arthroscopic surgery first then total shoulder replacement and 37 patients had the total shoulder replacement without prior arthroscopic shoulder surgery to measure the failure rates of the surgery.
- There were 4 patients (7.1%) who had failure, and failure rates did not differ significantly between the arthroscopic surgery first then total shoulder replacement (5.3%) and primary total shoulder replacement only group.
- Additionally, 2 patients underwent revision arthroplasty because of trauma.
- A total of 50 patients who did not experience failure (17 arthroscopic surgery first then total shoulder replacement and 33 primary primary total shoulder replacement) completed patient surveys at almost five years after their last surgery measures with no significant difference between the arthroscopic surgery first then total shoulder replacement and primary primary primary total shoulder replacement.
- Both groups improved significantly from preoperatively to postoperatively in all survery scores.
The conclusion of this research: “Patients with severe glenohumeral osteoarthritis who failed previous arthroscopic surgery benefited similarly from total shoulder replacement compared with patients who opted directly for total shoulder replacement.”
Who does reverse total shoulder replacement work for best? Glenohumeral osteoarthritis with intact rotator cuff.
A May 2024 study (8) reviewed the previously published data of patient outcomes following total shoulder replacement to determine patient satisfaction following the surgery at a minimum two-year follow-up.
- There were a total of 5234 patients and 5288 shoulders from the 45 included studies.
- The overall study population was 61.2% female and the average age was 71.1 years (range 23 being the age of the youngest patient and 99 being the age of the oldest patient).
- Overall patient satisfaction ranged from 77.7 to 87.8%, depending on patient satisfaction surveys.
- Patients with a diagnosis of glenohumeral osteoarthritis rated better satisfaction on all metrics when compared to patients with a diagnosis of cuff tear arthropathy or massive rotator cuff tear.
A March 2025 study (9) compared patient outcomes between anatomic total shoulder replacement and reverse total shoulder replacement. This study found anatomic total shoulder replacement significantly outperformed reverse total shoulder replacement in physical ability and range of motion, The wrote: “anatomic total shoulder replacement patients were seen as having a 40% chance of perceiving their shoulder as normal.”
The bone marrow stem cell procedure uses adult stem cells or mesenchymal stem cells.
References
1 Stanborough RO, Bestic JM, Peterson JJ. Shoulder Osteoarthritis. Radiol Clin North Am. 2022 Jul;60(4):593-603. doi: 10.1016/j.rcl.2022.03.003. PMID: 35672092.
2 Al-Mohrej OA, Prada C, Leroux T, Shanthanna H, Khan M. Pharmacological Treatment in the Management of Glenohumeral Osteoarthritis. Drugs & Aging. 2022 Feb;39(2):119-28.
3 Yamamoto N, Szymski D, Voss A, Ishikawa H, Muraki T, Cunha RA, Ejnisman B, Noack J, McCarty E, Mulcahey MK, Itoi E. Non-Operative Management of Shoulder Osteoarthritis: Current Concepts. Journal of ISAKOS. 2023 Jun 13.
4 Cooper BJ, Kesinger A, Welch GE, Carroll JM, Lutz A, Shanley E, Thigpen CA, Tolan SJ, Kissenberth MJ, Pill SG. Judicious use of corticosteroid injections prior to shoulder arthroplasty does not compromise outcomes at a minimum of 2 years following surgery. Journal of Shoulder and Elbow Surgery. 2024 Jun 1;33(6):S49-54.
5 Familiari F, Ammendolia A, Rupp MC, Russo R, Pujia A, Montalcini T, Marotta N, Mercurio M, Galasso O, Millett PJ, Gasparini G. Efficacy of intra‐articular injections of hyaluronic acid in patients with glenohumeral joint osteoarthritis: a systematic review and meta‐analysis. Journal of Orthopaedic Research®.
6 Kirschner JS, Cheng J, Creighton A, Santiago K, Hurwitz N, Dundas M, Beatty N, Kingsbury D, Konin G, Abutalib Z, Chang R. Efficacy of ultrasound-guided glenohumeral joint injections of leukocyte-poor platelet-rich plasma versus hyaluronic acid in the treatment of glenohumeral osteoarthritis: a randomized, double-blind controlled trial. Clinical Journal of Sport Medicine. 2022 Nov 1;32(6):558-66.
7 Nolte PC, Elrick BP, Arner JW, Ridley TJ, Woolson TE, Tross AK, Midtgaard KS, Millett PJ. Total shoulder arthroplasty after previous arthroscopic surgery for glenohumeral osteoarthritis: a case-control matched cohort study. The American Journal of Sports Medicine. 2021 Jun;49(7):1839-46.
8 Smith KL, Karimi A, Harlow ER, Gillespie RJ, Chen RE. Defining Patient Satisfaction after Reverse Total Shoulder Arthroplasty: A Systematic Review. Journal of Shoulder and Elbow Surgery. 2024 May 6.
9 Beleckas CM, Schodlbauer DF, Mousad AD, Levy JC. Evaluation of New Normal After Shoulder Arthroplasty: Comparison of Anatomic versus Reverse Total Shoulder Arthroplasty. Journal of Shoulder and Elbow Surgery. 2025 Mar 10.